Balance billing is a nice illustration of neoliberal transformation of medicine in the USA (see Neoliberal rationality) , when profits became
the primary motive and Hippocratic oath is completely forgotten. Like unnecessary operations (cardiac stent insertion is a classic example
here; see Overuse of Cardiac Stents)
this practice is designed to milk patients as much as possible, even if the service, such as ambulance was beyond their control. Some
states try to fight this practice, but their efforts are very limited (see below). It necessitate use of legal help for such cases.
You can't fight balance billing on your own.
In the United States, balance billing usually happens when you get care from a doctor or hospital that isn’t part of your health
insurance company’s provider network ("out of network" service) or doesn’t accept Medicare assignment. Some types of services such as
ambulances intentionally stay "out of network" to practice balance billing.
Practice known as “balance billing,” refers
to medical facilities ability to bill you for the remaining balance after your insurance pays its share. Because the specialist you
visited wasn’t bound by the contractual agreements of being in-network, they can legitimately bill you for the remaining balance. this
is a scam, but it is not prohibited by law. Also insurance companies often underpay for emergency services, so there is subtle interplay
between medical providers and insurance companies here. Insurance companies are a part of this dirty game.
Federal law does not currently protect consumers from balance billing. The Affordable Care Act (ACA) only guarantees that the health
plan must provide coverage for emergency services even if the providers are out of network. States take various approaches to protecting
consumers from balance billing. Nearly all states require HMO contracts to hold consumers harmless when they go to in-network providers;
a smaller share apply the same protections for PPOs.
As of 2016 only seven states—California, Colorado, Florida, Maryland, New Mexico, New York, and Texas—have some level of protection
of consumers (mainly for HMO) from certain types of balance billing (
insurance.pa.gov ):
Emergency Settings. In this scenario, the consumer has some type of medical emergency and is taken to a hospital for emergency care.6
Even if the consumer makes sure to go to a network hospital, there is no certainty that the emergency department (ED) is staffed
by network providers. In these situations, the consumer has little or no ability to choose a network or non-network provider. Most
consumers probably assume that the network hospital is staffed by network physicians and other health professionals. In reality,
this is not always the case. Data are not widely available to track how often these situations arise. But a recent study of networks
for the three largest insurers in Texas found that at least one of five in-network hospitals had no in-network
... ... ...
Table 1. Summary of Laws and Regulations Affecting Out-of-Network Balance Billing in Study States
California
Colorado
Florida
Maryland
New Mexico
New York
Texas
Hold harmless or provider prohibition on balance billing in emergency situations (Scenario 2)
Yes, for HMOs and some PPOs
Yes
Yes, for HMO plans
Yes, for HMOs and tied to assignment for PPOsc d
No
Yes
Yes, for HMOs and EPOsf
Hold harmless or provider prohibition on balance billing in surprise bills (Scenario 3)
No
Yes
Yes, for HMOsb
Yes, for HMOs and tied to assignment for PPOsc d
No
Yes, tied to assignmentd
Yes, for HMOs and EPOsf
Hold harmless or provider prohibition on balance billing in other situations (Scenario 4)
Noa
Yes
No
Yes, for HMOs and tied to assignment for PPOsc d
No
Yes, tied to assignmentd
Yes, for HMOs and EPOsg
State mediation or dispute resolution process
Yes, not much used
No
Yes, not much used
No
No
Yes
Yes, if more than $1,000
Disclosure
So if you ambulance is out of netwrok and you do not have Medicare Part B you are on the hook for a full billing amount
minus what you insurance paid. for example is billed amount is $5K and insurance paid $1.5K you owe $3.5K. Which is a lot of money.
They claim that the services were performed by an out of network provider. They (out of network providers) are not required to
accept any amount less than their billed rate. So, you owe the balance and your insurance company is not liable to pay for anything
more than what your policy says they are liable to pay.
Just as you prepared yourself for an outstanding bill before your appointment, you should double-check the math afterward. Medical
billing errors are common, and learning to spot the more frequently seen mistakes could save you some money.
Compare an itemized bill from your medical provider with the explanation of benefits (EOB) statement from your health insurance provider.
You should have received both of these after your insurance paid its portion.
Balance billing doesn’t usually happen with in-network providers or providers that accept Medicare assignment because, if they balance
bill you, they’re violating the terms of their contract with your insurer or Medicare. They could lose the contract, face fines, suffer
severe penalties, and even face criminal charges in some cases.
“The nonprofit UCR database, FAIR Health, Inc. was established in October 2009 to help ensure fairness and transparency in out-of-network
reimbursement. FAIR Health was created to serve as an independent, objective, and transparent source of healthcare reimbursement
data for consumers, insurers, healthcare providers, researchers, analysts, and policymakers.”7
It remains to be seen if FAIR Health turns out to be a more reliable database for calculating out-of-network reimbursement than Ingenix
because the FAIR Health began preliminarily providing cost estimates for common medical procedures on August 1, 2011 but is not yet
sufficiently populated with data to report estimates on all treatments and services.8
Aetna has taken a more direct approach by filing lawsuits against out-of-network providers who submit what
it believes are excessively large claims. The lawsuits are intended to signal that “billed charges have to be based on reasonable
factors that make sense in the marketplace.”15 As a matter of policy, Aetna attempts to insulate
its enrollees from balance billing by paying out-of-network physician claims in full.16
Hospitals themselves can choose to prohibit facility-based physicians from engaging in balance billing for any
services performed on-site and requiring all physicians seeing patients at the hospital to contract with all payors with which the
hospital contracts as a condition of privileging. Other hospitals may choose to notify affected patients upon admission that
they may be financially responsible for some services provided during their stay and attempt to persuade physicians to reduce balance
bills.
Conclusion
A satisfactory methodology for adequately compensating out-of-network physicians has yet to be agreed upon. Whatever solution or
variety of solutions is found, hopefully patients will no longer find themselves surprised and dismayed to receive balance bills
for services they perceived to be fully covered by their health insurance plans.
Patients receiving emergency medical care would no longer get surprise medical bills from providers outside their insurance network
under a rule issued Thursday by the Biden administration.
The long-awaited rule is the first to follow the so-called No Surprises Act, passed in December 2020 by Congress that sought
to protect patients from receiving significant medical bills when they are unwittingly treated by an out-of-network doctor, lab,
or other type of provider.
The rule seeks to implement key parts of the legislation protecting patients from being billed by out-of-network doctors who provide
treatment at in-network hospitals, as well as protecting them from surprise bills for both emergency and nonemergency care. The
interim final rule will
undergo 60 days of public comment and largely go into effect on Jan. 1, 2022, when the law takes effect.
"No patient should forgo care for fear of surprise billing," said Health and Human Services Secretary Xavier Becerra in a statement.
"Health insurance should offer patients peace of mind that they won't be saddled with unexpected costs."
Congress and policy makers
have sought to tackle surprise medical bills because patients are paying more out-of-pocket for their care, and many out-of-network
charges can occur when patients are unaware that they are being treated by a provider who isn't covered by their health insurance.
Out-of-network charges have added to medical debt and rising out-of-pocket payments for consumers: An April 2021 study in the
journal Health Affairs found that patients receiving a surprise out-of-network bill for emergency physician care paid more than 10
times as much as in-network emergency patients paid out-of-pocket .
The interim final rule is expansive. Emergency services, regardless of where they are provided, would have to be billed at lower,
in-network rates without requirements for prior authorization.
The rule also bans higher out-of-network cost-sharing, such as copayments, from patients for treatment they receive either
in an emergency or nonemergency situation. Under the rule, any coinsurance or deductible can't be higher than if such services were
provided by an in-network doctor.
The interim final rule also stipulates that patients can't be charged out-of-network for "ancillary" care, which can happen when
an out-of-network anesthesiologist or assistant surgeon provides treatment at an in-network hospital.
Regulations that will be released at a later time will implement a procedural process so medical providers and insurers can arbitrate
out-of-network payment disputes, a solution that was so contentious it threatened to scuttle passage of the No Surprises Act. Insurers
raised concerns that arbitration could put them at a disadvantage and instead favored linking out-of-network reimbursement to a benchmark
rate.
The legislative fight over the No Surprises Act that spurred the interim rule was contentious. The American Medical Association
and some state medical associations worried it could financially hurt small physician practices that were still reeling from the
pandemic. The American Hospital Association supported the arbitration provision but raised concerns about the possibility for uneven
enforcement of the law.
The bill will lead to "dangerous, unintended consequences, right in the middle of a surging pandemic," according to a Dec. 15,
2020, letter to then-Senate Majority Leader Mitch McConnell (R., Ky.) from conservative groups such as Action for Health.
Cost-sharing includes deductibles, copayments paid at the time of treatment, and coinsurance, which is the percentage of a bill
that consumers pay that isn't covered by insurance. Patients are paying increasingly more for their own care because cost-sharing
has increased over time, research shows. Most workers also face additional cost-sharing for a hospital admission or outpatient surgery.
Sixty-five percent of workers with employer-sponsored coverage have coinsurance and 13% have a copayment for hospital admissions,
according to a 2020 survey by the Kaiser Family Foundation.
Out-of-network charges from anesthesiologists, pathologists, radiologists and assistant surgeons increase spending by $40 billion
annually, according to researchers at the Yale School of Public Health.
Congress in its legislation sought to protect patients from unknowingly receiving care from an out-of-network provider. To that
end, the rule bans other out-of-network charges without advance notice.
The regulations issued Thursday will take effect for healthcare providers and facilities Jan. 1, 2022. For group health plans,
health-insurance issuers and Federal Employees Health Benefits program carriers, the provisions will take effect for plan, policy
or contract years beginning on or after Jan. 1, 2022.
Please not that stent insertion is often unnecessary procedure performed not to save the life of the patient but to earn money.
The system is criminal indeed.
Non-profits hospitals those day are also governed by Wall-street sharks.
Please note that Abdominal CT scan with insurance like CIGNA would cost you $300-$600 out of the pocket depending on the
facility.
Notable quotes:
"... abdominal and pelvic scan at Avera St. Luke's cost $6,422, the highest out of a wide range of rates the Avera hospital charges for that service ..."
"... Some dominant local and regional nonprofits, including Mass General Brigham, based in Boston, and Avera, based in Sioux Falls, S.D., billed the uninsured at their general hospitals some of their highest prices while also setting some of the most restrictive financial-aid policies for free care nationwide, according to tax filings, Turquoise data and patients' medical bills. ..."
"... "It's really criminal, the mess that our current system is in," said Mary Daniel, chief executive of ClaimMedic, which helps patients negotiate payment with hospitals. "It is a deliberate attempt for these hospitals to gouge the uninsured." ..."
"... for expensive procedures like angioplasty and drug-coated stenting, the difference in the cash price within a single county can be over $100,000. ..."
"... The cash prices for patients who must pay for their own care can be equal to the sticker prices or sometimes represent a percentage lopped off that top rate. Sometimes, those cash rates are also applied to people who have some form of insurance but get a service that the insurance doesn't cover. ..."
"... The quarter of hospitals with the most generous free-care policies write off the entire bill for those with monthly incomes under about $2,600 a month, and even up to roughly $6,400 a month, for a one-person household, the Journal found. ..."
"... Those that rank in the quarter of hospitals with the most-restrictive policies draw the line at or below about 160% of the federal threshold for poverty, disqualifying for free care patients with monthly income of more than around $1,700 for a one-person household, according to a Journal analysis of nonprofit hospital tax filings. ..."
"... A patient paying cash at the hospital for the stenting procedure is charged $84,792. Local insurer Fallon Health spends $36,755 for the procedure under one of its health-maintenance organization plans. A Medicare insurance plan from Aetna, part of CVS Health Corp. , pays $16,648. ..."
"... Patients who don't qualify for financial aid at nonprofit hospitals also aren't protected by pricing limits under federal law. The Affordable Care Act requires nonprofit hospitals to cap prices for patients who qualify for financial aid. ..."
"... Hospitals apply financial aid and discount policies inconsistently, say consumer advocates and patients. Offers may be one-time-only, or discounts may emerge only when a skilled negotiator is pushing for them. ..."
"... In January 2018, Joannie Berthiaume spent two days at Broward Health Imperial Point hospital in Fort Lauderdale, Fla., and got emergency surgery to remove her appendix. She was uninsured and the hospital charged Ms. Berthiaume its highest prices. Her bill totaled about $42,000, including a $6,033 abdominal CT scan. For that same scan, an Aetna subsidiary gets a 24% break, according to the newly public data from Broward Health. That discount would have meant a fee of around $4,600 for the scan, based on the price charged in 2018. ..."
"... "If you charge me $42,000 and your costs are justified, how can you knock it in half in a matter of minutes," Ms. Berthiaume says. "You must be overcharging." ..."
"... High cash prices inflate bills that uninsured patients often struggle to pay. Hospitals collected 5% of the amount they billed uninsured patients before writing off bills after a year of seeking payment, according to Crowe LLP, an accounting, technology and consulting firm, based on an analysis of 600 client hospitals. That is compared with collecting 40% of bills sent to patients with insurance for amounts owed under deductibles, copays and other out-of-pocket costs, based on a separate analysis by Crowe of about 1,500 hospitals. ..."
"... Hospitals closely track their "payer mix," or the mix of patients with commercial insurance, Medicare, Medicaid and the uninsured, who might be unlikely to ever pay for their treatment. That could play a role in how hospitals set prices. ..."
"... Resolve also offered about $8,000, or slightly more than the company estimated Medicare would pay, for Mr. Macias's $24,800 emergency-room bill at Avera St. Luke's, Mr. Pan said. The hospital said no, and despite denying financial aid, offered to reduce the bill by 50%, Mr. Pan said. The amount excluded another $34,994 he owes Avera's heart hospital. ..."
"... Have you or someone you know faced a challenging hospital billing situation? Tell us about your experience in the form below. ..."
The 32-year-old's abdominal and pelvic scan at Avera St. Luke's cost $6,422, the highest out of a wide range of rates the Avera
hospital charges for that service based on the new data. The price billed to Mr. Macias was roughly three times the best deal negotiated
by an insurance company.
Another scan of his chest came to $4,194, approximately $280 to $2,800 more than any prices negotiated between St. Luke's and
an insurer. The prices for identical scans performed at Avera's heart hospital were also among the highest that the hospital charged. His total hospital bills came to $59,800.
... ... ...
Services including emergency-room visits, imaging scans and procedures such as an angioplasty and stenting often performed on
heart-attack patients have been identified by researchers and federal data as commonly needed in emergencies by those without insurance.
The Journal analysis looked at the 1,550 hospitals in the Turquoise data that released both insurance and cash-payment rates.
Among the Journal's findings:
Hospitals routinely bill uninsured patients at their highest rates. About 21%, or 319, of the hospitals did so for the majority
of the services included in the analysis. At 171 of those hospitals, the cash rate was higher than all of the rates billed to
insurers, or tied for the highest rate, for every service in the analysis. That was true at some hospitals owned by major systems
including Sanford Health and Yale New Haven Health System.
On average, across the 1,166 hospitals that included rates for Medicare Advantage plans in their disclosures, the fees for
uninsured patients were 3.6 times the average rates paid by the Medicare Advantage plans. Medicare rates are typically set by
the government to at least cover hospital costs and are considered a baseline for comparing prices. Rates for Medicare Advantage
plans, which are administered by private insurers, are generally close to these mandated prices.
Some dominant local and regional nonprofits, including Mass General Brigham, based in Boston, and Avera, based in Sioux
Falls, S.D., billed the uninsured at their general hospitals some of their highest prices while also setting some of the most
restrictive financial-aid policies for free care nationwide, according to tax filings, Turquoise data and patients' medical bills.
Cash prices, which haven't been available publicly to help patients choose where to seek medical care, often vary widely even
among hospitals in the same county. In the 270 counties where at least two hospitals have disclosed their cash prices, the average
spread between the lowest and highest rates for a complex emergency-room visit is $1,852.
In Shelby County, Tenn., home to Memphis, the spread for that type of ER visit is $2,054. It would cost an uninsured patient $884
at any of the three Baptist Memorial Health Care hospitals; $1,480 at Regional Medical Center; $2,653 at Saint Francis Hospital-Memphis;
and $2,938 at Saint Francis Hospital-Bartlett.
... ... ...
Hospitals that offer additional discounts for the uninsured don't always automatically make the cuts to patient bills, leaving
cash-pay patients with significantly higher charges, the Journal found. It can take long negotiations, often by hiring lawyers or
professional advocates, to bring about reduced charges.
... ... ...
Those discounts slash bills by an average of 85% off its top price, the company said in a recent statement to the Journal. But
patients must apply to receive the discount. The vast majority of cash prices for emergency services at Tenet hospitals reviewed
by the Journal instead reduced bills by 20% to 30%.
"It's really criminal, the mess that our current system is in," said Mary Daniel, chief executive of ClaimMedic, which
helps patients negotiate payment with hospitals. "It is a deliberate attempt for these hospitals to gouge the uninsured."
The differences between the prices for uninsured people and insurance companies can be wide.
At Ephraim McDowell Regional Medical Center in Danville, Ky., an uninsured person getting a stent after a heart attack could be
billed around $66,226 for the procedure. An Anthem Inc.
health-maintenance organization plan would pay just $17,895 at the hospital, and the insurer's Medicare plan even less -- $12,445.
Ephraim McDowell Health said the cash prices are the highest rates but that it offers discounts and bill forgiveness for those
who qualify for financial assistance. In a written statement, the hospital system said, "it is rare that an uninsured patient would
pay the total gross charge amount due to the variety of financial assistance programs available."
Eligibility under the program cuts off at three times the federal poverty level, according to the hospital system, which is an
annual income of $38,640 for a single person.
Prices typically haven't been publicly available before now. Yet for expensive procedures like angioplasty
and drug-coated stenting, the difference in the cash price within a single county can be over $100,000.
The reasons for high cash prices are complex and, even to many healthcare experts, baffling.
Hospitals typically have a sticker price, often called the "chargemaster" price, that can be the starting point for negotiations
with insurers. Discounts off that sticker price tend to be steeper for those that bring large volumes of patients. Insurance plans
offered under government programs like Medicare and Medicaid get even lower rates, tied to prices mandated by federal and state agencies.
The cash prices for patients who must pay for their own care can be equal to the sticker prices or sometimes represent a percentage
lopped off that top rate. Sometimes, those cash rates are also applied to people who have some form of insurance but get a service
that the insurance doesn't cover.
Will Fox, who advises hospitals on pricing as an actuary with Milliman Inc., says hospitals often keep cash prices above the rates
negotiated by big insurers.
"They don't want to give away too much of a discount because they really want the best discounts to go to these larger volume
negotiated insured rates," he said. "Somebody walking off the street, we'll give you a 20% discount, but we're going to give our
favorite customer, who sends us millions or even billions of dollars in business, we're going to give them a much bigger discount."
Yale New Haven Health offers cash prices that represent a discount off sticker rates, but it keeps them above all of the prices
negotiated by insurers, says Pat McCabe, the system's senior vice president of finance. "We didn't want there to be that tension,
for an insurer to look at that data and say, 'you're providing better rates to uninsured patients than you are to our insureds, how
do we justify that to our members and/or employer partners?' "
For individuals who struggle to pay, financial aid is hard to get at some hospitals with high cash prices, the Journal analysis
found. That is true even among the nearly 3,000 nonprofit hospitals that get tax breaks on the condition they give back to the community.
Hospitals typically set household income limits for financial aid, with free care for patients below a cutoff.
The quarter of hospitals with the most generous free-care policies write off the entire bill for those with monthly incomes
under about $2,600 a month, and even up to roughly $6,400 a month, for a one-person household, the Journal found.
Those that rank in the quarter of hospitals with the most-restrictive policies draw the line at or below about 160% of the
federal threshold for poverty, disqualifying for free care patients with monthly income of more than around $1,700 for a one-person
household, according to a Journal analysis of nonprofit hospital tax filings.
Brigham and Women's Hospital, affiliated with Harvard Medical School, falls in this most-restrictive group, with income cutoffs
for free care at $1,610 a month for a one-person household. For 12 of 17 emergency services at Brigham and Women's reviewed by the
Journal, its highest rates are for uninsured patients, and insurance companies pay significantly less.
Brigham and Women's Hospital, in Boston, Mass., is among the group of nonprofit hospitals with the most-restrictive income cutoffs
for free care.
A patient paying cash at the hospital for the stenting procedure is charged $84,792. Local insurer Fallon Health spends $36,755
for the procedure under one of its health-maintenance organization plans. A Medicare insurance plan from Aetna, part of
CVS Health Corp. , pays $16,648.
Mass General Brigham, the system that includes Brigham and Women's, said in a written statement it has policies to prevent
someone without insurance from paying full price.
Some hospitals, including Brigham and Women's, also partially discount patients' bills for some who earn too much for free care.
Others write off bills that are large relative to a patient's income. But policies vary widely. The most-restrictive quarter of hospitals
cut off discounts at 2.5 times the federal poverty level, the Journal found.
Patients who don't qualify for financial aid at nonprofit hospitals also aren't protected by pricing limits under federal
law. The Affordable Care Act requires nonprofit hospitals to cap prices for patients who qualify for financial aid.
Hospitals apply financial aid and discount policies inconsistently, say consumer advocates and patients. Offers may be one-time-only,
or discounts may emerge only when a skilled negotiator is pushing for them.
In January 2018, Joannie Berthiaume spent two days at Broward Health Imperial Point hospital in Fort Lauderdale, Fla., and
got emergency surgery to remove her appendix. She was uninsured and the hospital charged Ms. Berthiaume its highest prices. Her bill
totaled about $42,000, including a $6,033 abdominal CT scan. For that same scan, an Aetna subsidiary gets a 24% break, according
to the newly public data from Broward Health. That discount would have meant a fee of around $4,600 for the scan, based on the price
charged in 2018.
Ms. Berthiaume, who is Canadian but was living in Florida at the time of her illness while finishing graduate school, went in
person to Broward Health to ask about the bill. She was told it could be cut in half, to about $21,000 total -- if she paid in full
right then. Ms. Berthiaume, then working in a part-time bookkeeping job, says she couldn't do that. The hospital later continued
to seek the full amount, including in letters sent by a law firm and reviewed by the Journal.
"If you charge me $42,000 and your costs are justified, how can you knock it in half in a matter of minutes," Ms. Berthiaume
says. "You must be overcharging."
Ms. Berthiaume hired attorney Jacqueline Grady to negotiate on her behalf, and in October 2019 the hospital offered to accept
$20,000, in addition to $2,000 she had already paid, if she paid within 16 days. Ms. Berthiaume declined.
Broward Health declined to comment on the details of Ms. Berthiaume's case, although she signed a consent form allowing the hospital
system to do so. The hospital system said that U.S. citizens and people with a permanent U.S. residence who come to its hospitals
for unplanned care, and don't qualify for its financial assistance program, are offered a discounted rate.
In the pricing data files Broward Health has disclosed under the federal transparency requirement, the cash prices are shown as
Broward's highest rates. However, the hospital system pointed the Journal to a consumer tool on its website that displays lower prices
for self-pay patients. Broward Health said in a written statement that the tool "provides the most current pricing for consumers,"
and "discounted prices may not be reflected" in the data files. The system didn't respond to questions about the reasons for the
discrepancy.
High cash prices inflate bills that uninsured patients often struggle to pay. Hospitals collected 5% of the amount they billed
uninsured patients before writing off bills after a year of seeking payment, according to Crowe LLP, an accounting, technology and
consulting firm, based on an analysis of 600 client hospitals. That is compared with collecting 40% of bills sent to patients with
insurance for amounts owed under deductibles, copays and other out-of-pocket costs, based on a separate analysis by Crowe of about
1,500 hospitals.
Hospitals closely track their "payer mix," or the mix of patients with commercial insurance, Medicare, Medicaid and the uninsured,
who might be unlikely to ever pay for their treatment. That could play a role in how hospitals set prices.
For Mr. Macias, debt from Avera hospitals plus other bills related to his November hospitalization amount to about 75% of his
annual income, according to Resolve Advocates, one of a growing number of companies that patients hire to negotiate hospital medical
bills on their behalf.
Mr. Macias, a superintendent for a construction company, suffered a potentially life-threatening tear in the lining of his largest
artery. He said he has largely recovered.
Avera's hospital in Aberdeen charged him the highest price for some emergency room services, according to a review of medical
bills for Mr. Macias and the Journal's analysis of Avera's negotiated rates with insurers.
Avera in some cases has multiple contracts with a single insurer and said the prices it made public are the average price it charges
an insurer for each service.
The Avera Heart Hospital of South Dakota, in Sioux Falls, gave Mr. Macias a 20% discount. Even with the discount, some of the
heart hospital prices were in the top third of what the hospital charged patients with insurance for some services.
Mr. Macias, a superintendent for a construction company, earned too much for free care at Avera, where the income cutoff is among
the lowest nationally for nonprofit hospitals, ranking in the bottom quarter, according to the Journal analysis.
But he appears to qualify for other financial assistance, such as a partial discount based on income or because Mr. Macias's medical
debts are large when compared with his household finances, said Resolve's chief executive, Braden Pan.
Avera rejected the request, saying that Mr. Macias could have had workplace health benefits but didn't enroll, according to Resolve.
Mr. Macias said in an interview that he missed the sign-up after miscommunication with his former employer. Buying insurance in the
marketplace was too costly, he said.
Avera also rejected an appeal, after factoring in his assets alongside his income, according to Resolve. Mr. Macias said he needs
his years of savings for a house down payment.
Resolve also offered about $8,000, or slightly more than the company estimated Medicare would pay, for Mr. Macias's $24,800
emergency-room bill at Avera St. Luke's, Mr. Pan said. The hospital said no, and despite denying financial aid, offered to reduce
the bill by 50%, Mr. Pan said. The amount excluded another $34,994 he owes Avera's heart hospital.
Mr. Macias, citing his unhappiness about the fight, told the Journal he wouldn't give Avera permission under federal privacy laws
to speak about his interactions with it.
"Health care delivery comes with a cost -- and when individuals have the means to pay, it allows us resources to help those
most in need," Lindsey Meyers, a spokeswoman for Avera, said in a written statement. "We have thoroughly reviewed the case you
have mentioned and identified that all processes were followed as described, and we made every effort to work with the patient."
Mr. Macias said he has largely recovered with new blood-pressure medication and months of rehab exercises he devised on his own.
He now lives in Austin, Texas, with his fiancée and their children, ages 6 and 3. Avera's debt collectors call constantly, he said.
"They're still blowing me up."
"... While general medical care is single payer in Canada, dental services are not. For major work on teeth, it is cheaper to fly to Mexico. The downside is for Mexicans -- such practices will drive the costs up in Mexico. ..."
"The art of medicine consists of amusing the patient while nature cures the disease."
"No, I mean I'm sorry that you've inherited such a miserable, collapsing Old Country. A place where rich
Bankers own everything, where you've got to be grateful for a part-time job with no benefits and no retirement
plan, where the most health insurance you can afford is being careful and hoping you don't get sick
Cory Doctorow;
Homeland
"Until fairly recently, every family had a cornucopia of favorite home remedies–plants and household items
that could be prepared to treat minor medical emergencies, or to prevent a common ailment becoming something much
more serious. Most households had someone with a little understanding of home cures, and when knowledge fell
short, or more serious illness took hold, the family physician or village healer would be called in for a
consultation, and a treatment would be agreed upon. In those days we took personal responsibility for our
health–we took steps to prevent illness and were more aware of our bodies and of changes in them. And when illness
struck, we frequently had the personal means to remedy it. More often than not, the treatment could be found in
the garden or the larder. In the middle of the twentieth century we began to change our outlook. The advent of
modern medicine, together with its many miracles, also led to a much greater dependency on our physicians and to
an increasingly stretched healthcare system. The growth of the pharmaceutical industry has meant that there are
indeed "cures" for most symptoms, and we have become accustomed to putting our health in the hands of someone
else, and to purchasing products that make us feel good. Somewhere along the line we began to believe that
technology was in some way superior to what was natural, and so we willingly gave up control of even minor health
problems."
Karen Sullivan;
The Complete Family Guide to Natural Home Remedies: Safe and Effective Treatments for
Common Ailments
No, I haven't abandoned Uncle Volodya, or shifted my focus to American administration; what follows is a guest
post on the American healthcare system, by our friend UCG. As I've mentioned before – on the occasion of his
previous guest post, in fact – he is an ethnic Russian living in the Golden State.
As an American in America, naturally his immediate concern is going to be healthcare in America; but there are
lessons within for everyone. Don't get me wrong – doctors have done a tremendous amount of good, and medical
researchers and many others from the world of medicine have made tremendous advances to which many of us owe their
lives. Sadly, though, once a field goes commercial, the main focus of attention eventually becomes profit, and
there are few endeavors in which the customer base will be so desperate. While there are obvious benefits to
'socialized medicine' such as Canada enjoys and American politicians scorn as 'Commie' – enough to earn the
admiration of many – it results in such a backlog for major operations that those who don't like their chances of
dying first, and have the money or can somehow get it, often flee to America, where you can get a good standard of
medical care without running out of time waiting for it.
Without further ado, take it away, UCG!!
Healthcare in America
This article is my opinion. My hope is that others will do their own research on America's Healthcare Industry,
because this is an issue that needs to be addressed, and for this article to be a mere starting point in this
research. The reason for my citations is so that you, the reader, can verify them. Once again, this is my opinion.
I write this in the first paragraph, so that I can avoid stating "in my opinion" before every sentence.
I tore my ab wall a month ago and didn't think much of it until my pain kept worsening. I went to an
immediate care facility to rule out a hernia (I had all the symptoms) and they told me to get to ER ASAP. I go to
the ER and they give me a CT scan and one x-ray and say it's not a hernia and let me go. Fast forward to today and
I got a bill for $9,200 and $3,900 of it is out of pocket. $9,200 for two tests???? No pain meds were
administered; it was literally those two tests. What should I do to contest it? I will be calling tomorrow to
demand an itemized bill, but is there anything else I should do in the meantime?
All of these took me a few minutes on Google to find, and another few minutes to post. The reason I chose that
reddit, is because one of the readers offered an ingenious solution:
Next time you hurt yourself – book a
return ticket to NZ – go to accident and emergency, say you're a tourist and you hurt yourself surfing, pay
nothing – fly home and pocket $8,000 in spare change.
If that was me, I'd spend at least $2,000 on tourism in
New Zealand. You guys have that system, so you clearly deserve the money! Anyone interested in a startup?
But I am not done with examples just yet. Shana Sweney
described her experience in the emergency room
:
I delivered in 15 minutes. During that time, the
anesthesiologist put a heart rate monitor on my finger and played on his phone. My bill for his services was
$3,000. $200/minute. I talked to the insurance company about it – and since I ran my company's benefit plans, I
got a little further than most people, but ultimately, that was what their contract with the hospital said so
that's what they had to pay. Regardless of if he worked 15 minutes or 3 hours. Similarly, my twins were born
prematurely and ended up in the NICU for 2 weeks. While the NICU was in-network for my insurance, for some
mysterious reason, the neonatologists that attended the NICU were out of network. I think that bill was $16k and
they stopped by to see each kid for an average of about 30 min/day.
$984.157 billion. That's $984,157,000,000. That is how much money I believe the United States wastes on
Healthcare. Not spends; wastes. As in money down the drain. The astute reader figured out that equates to
five percent of America's 2016 GDP
. Said reader is
absolutely correct. How did I estimate such a gargantuan amount?
According to the OECD data
,
in 2013 the United States spent 16.4 percent of its GDP on Healthcare; the two next biggest spenders, Switzerland
and the Netherlands spent 11.1 percent. Even if one was to give the United States the benefit of doubt, and claim
that the United States healthcare is just as efficient as that of Switzerland or the Netherlands – which is most
likely not true according to
an
article from Business Insider
, but even if it was – that meant that the United States wastes 5.3% of its GDP
on healthcare. Wastes. I just want to make sure that the amount of this alleged legalized corruption, which will
most likely reach a trillion dollars by 2020, is noted.
Let me place those funds into perspective: it's almost as much as the amount that
the rest of the World spends
on the military, combined
. The SCO member states, including China, Russia, India, and Pakistan spent
roughly $360 billion on the
military
. The wasted amount is equivalent to the GDP of Indonesia, and
greater than the GDP of Turkey
or Switzerland
. In 2016, the US Federal Government spent $362 billion, or 36.8% of the wasted amount,
to run all Federal Programs
, including the Department
of Education and NASA, with the exception of Social Security, Medicare/Medicaid, Veteran's Affairs, the military,
and net interest on the US debt. All other Federal Programs were covered with the $362 billion. The US Federal
Debt
stands at $20.4 trillion
, meaning that the debt can be paid off in
30 years, merely if the Healthcare Waste is eliminated.
But why stop there? The US Housing Crisis started partly because loans were allowed to be taken out without the
20% down payment. Could this funding, if applied directly to the housing market, stop the 2008 Great Recession?
Absolutely, and
all the Federal Government had
to do
was to gear these funds towards down payment on subprime mortgage loans to meet the 20 percent barrier.
I can go on and on about what can be accomplished, like making collegiate attendance free, or at least very
inexpensive, or drastically improving the quality of education, paying off the national debt, reinvesting into the
economy, reinvigorating the rural sector, and so on, and so forth. A trillion dollars is a lot of money.
Lobbyists, the Media and the Waste
Any guess how much was spent on lobbying by the Healthcare, Insurance, Hospitals, Health Professionals, and
HMOs?
How about 10.5 billion dollars?
I knew
that was your guess! That's a lot of money, and that does not include "speaking fees", or when a politician who
constantly made calls beneficial to the Healthcare Lobby gets $150,000 to speak in front of an audience after they
retire from politics. Obama made a speech in front of Wall Street,
netting $400,000
. And by pure coincidence,
only one
Wall Street Broker was jailed
as a result of the scandal. That $10.5 billion is just a tip of the iceberg,
because "speaking fees" are notoriously hard to track, and not included in said amount.
Obama genuinely tried to reform US Healthcare to the Swiss Model. He was going to let Wall Street slide, he was
going to let Neocons conduct foreign policy, just please, let him have healthcare! First, the lobbyists laughed in
his face. Second, they
utilized the Blue Dog Coalition
to block Obama's attempt at Healthcare Reform, until it was phenomenally
nerfed, and we have the disaster that we have today. As a result, Obama's Legacy, Obamacare is having major
issues, including the rise of racism.
Obamacare helped the poor, (mostly minorities,) at the expense of the middle class, (mostly whites,) thus
transferring funding from whites to minorities. While the intent was not racial, it is being
called out
as racial by the mainstream media
. This probably suits the lobbyists, because if the debate is about racism,
one cannot have a genuine discussion about Healthcare Reform.
Racism strikes both ways. Samantha Bee came out with a
"fuck you
white people"
message right after the election. Jon Stewart, without whom she probably wouldn't have her own
show, pointed out that it was simply economics,
like the
healthcare insurance premium increase
, that brought Donald Trump to power. Interestingly enough, James
Carville made the same argument when Bill Clinton beat George Bush, but when Hillary Clinton lost, Carville was
quick to blame Russia. These delusions on the Left are letting the Right mobilize stronger than ever before. And
all of this takes away from the Healthcare Debate.
In an attempt to blame Trump's Election on white racism, rather than basic economics, numerous outlets simply
fell flat. For instance,
Eric Sasson writes
:
white men went 63 percent for Trump versus 31 percent for Clinton, and white women went
53-43 percent. Among college-educated whites, only 39 percent of men and 51 percent of women voted for Clinton
What's more, these people hadn't suffered under Obama; they'd thrived. The kind of change Trump was espousing
wasn't supposed to connect with this group.
Let's start with the banks. Medical students graduate with an average of
$416,216 in student debt
.
The
average interest rate
on said loan is
seven percent. Roughly 20,055 students
go through this
program, per year
. Presuming a twenty year loan, the banks are looking at about $7.185 billion in interest
payments. It really is a small fraction of the cost. Prescription drug prices are another story. In 2014, Medicare
spent $112 billion on
medicine for the elderly
. Oh la la! Cha-ching. I would not be surprised if at least half of that was wasted
on drug price inflation. You know the health insurance companies? It's a great time to be one, since profits are
booming – to the tune of
$18 billion in
projected revenue
for 2017.
Of course the system itself is quite wasteful, with needless hours spent on paperwork, claim verification,
contractual review, etc, etc, etc. Humana's revenue was
$54.4 billion
,
Aetna's was
$63.2
billion
, Anthem's was
$85 billion
,
Cigna's was
$39.7
billion
, and UnitedHealth's was
$184.8 billion
. Those
are just the top five companies. None of them ia a mom-and-pop shop or small business store. Do any of these
insurers support Obamacare? Even if they do, it is
without much enthusiasm
. They are leaving, and leaving quite quickly. Thirty-one percent of American counties
will have
just one healthcare insurer
. Welcome to a monopoly that is artificially creating itself. And despite the
waste,
28.2 million
Americans remain uninsured
. Mission accomplished!
Who else benefits? Those who hire illegal immigrants instead of American workers, since illegal immigrants cost
the United States roughly
$25 billion
in Healthcare spending
. Meanwhile those who hire them can avoid certain types of taxes and not have to cover
their Healthcare; communism for the rich, capitalism for the rest of us. Of course that is just a rough estimate,
since this spending is also quite hard to track.
The Future
The problem with changing Healthcare is that too many people have their hands in the proverbial pie. There is
not a single lever of power that isn't affected by Healthcare, and most of the levers that are affected, benefit
quite a bit. Insurance companies will fight to the death, because Universal Healthcare will be their death knell.
Banks will defend it, because who doesn't want to make billions from student loans? Medical schools too – since it
lets them charge higher and higher tuition. Pharmaceutical companies can use the increase in Healthcare
expenditure to justify their own price hikes, even though a major reason for those price hikes is artificial
patent based monopoly.
What is an artificial monopoly? In my opinion, it's when a patent is utilized to prevent competitors from
manufacturing the same exact drug. In less than a decade, the price of Epi-Pen soared from $103.50 to $608.61.
When asked the justify said increase,
one of
the reasons provided by the CEO
was that
the price went up because we were making investment; as I said,
about $1 billion over the last decade that we invested in the product that we could reach physicians and educate
legislatures.
"Reaching" doctors and legislators; I wonder, how was said "education funding" spent? According
to US News, a website that is extremely credible when it comes to internal decision making within the United
States,
drug companies have long courted doctors with gifts
, from speaking and consulting fees to educational
materials to food and drink. But while most doctors do not believe these gifts influence their decisions about
which drugs to prescribe, a new study found the gifts actually can make a difference – something patient advocates
have voiced concern about in the past. Do you feel educated? Would you feel more educated if I paid you a
$150,000 consulting fee? What about $400,000? What? It's just consulting; no corruption here!
Everyone knows that this is going on. But there is not going to be change. Why not? The same reason that there
was not change with Harvey Weinstein, until Taylor Swift came along. Remember how I said that almost everyone has
their hands in the Healthcare Pie? It was not much different with Weinstein. Scott Rosenberg explained
why it took so long for people to speak out against Harvey
, and the reasons were numerous. First, Harvey gave
many people their start in Hollywood, and treated all of his friends like royalty. That drastically increased
their loyalty. Second, he ushered the Golden Age of the 1990s, with movies like Pulp Fiction, Shakespeare in Love,
Clerks, Swingers, Scream, Good Will Hunting, English Patient, Life is Beautiful – the man could make phenomenal
movies. Third, even if one was willing to go against his own friends, workers, mass media, and so on, there was no
one to tell. There was no place to speak out. Fourth, some of the victims took hefty settlements.
That fourth reason enabled mass media to portray rape victims as gold diggers. Rape Culture is alive and well.
In California, a Judge
gave minimal sentencing to a convicted rapist
, because he was afraid a harsher sentence would damage the
rapist's mental psyche for life. Uh dude, from one Californian to another, he, uh, raped. His mental psyche is
already damaged; for life. That's the kind of pressure that Rose McGowan had to deal with. She had
a
little kerfuffle with Amazon
, and she thinks it was partially because of Harvey Weinstein. How many times had
the word "socialism" been thrown around to describe Universal Healthcare? Switzerland has it – are they Socialist?
Enter Taylor
Swift
. In order to destroy allegations that women are filing sexual harassment claims as gold diggers, she
sued her alleged sexual assaulter for a buck; one dollar. She won. Swift stated that the lawsuit was to
serve
as an example to other women who may resist publicly reliving similar outrageous and humiliating acts.
On top
of that, Weinstein was no longer as popular as he used to be, and an avenue to tell the story, an outlet was
created. The additional prevalence of the internet caused the stories of Weinstein's sexual abuse to leak. Within
a month, the giant fell.
Something similar is needed to change Healthcare in America. But until that comes along, racism will increase,
the cost of Healthcare will rise, emergency room costs will most likely double every ten years, and the future
remains bleak. As if that was not enough, more and more upper class Americans, (like yours truly,) are seeking
treatment abroad. It cost me less money to lose five weeks of wages, spend three weeks partying in Eastern Europe,
(Prague to be more specific,) after my two weeks of treatment, buy a roundtrip plane ticket, and stay in a five
star, all-inclusive hotel, than the cost of the same treatment in the US. If anyone wants to utilize this as a
startup – let me know!
Of course its effects on Healthcare will hurt, since it is a huge chunk of business that will be traveling
across the Atlantic. But what can be done to stop it? One cannot stop Americans from traveling to other countries.
One cannot force the poor to work for free. Perhaps this is the change that is needed to make those who benefit
from the Healthcare Waste realize that this cannot continue. Perhaps not. What we do know, is that Obamacare
insured the poor,
at
the expense of the middle class
. And that is regarded as a failure in America.
"In trying to show that he was successfully managing the Obamacare rollout, the
president last week staged a high-profile White House meeting with private health insurance executives -- aka
Obamacare's middlemen. The spectacle of a president begging these middlemen for help was a reminder that
Obamacare did not limit the power of the insurance companies as a single-payer system would.
****The new law instead cemented the industry's profit-extracting role in the larger health system -- and it
still leaves millions without insurance."*** (THAT is the Achille's lower torso of the ACA)
Exactly! That's why I stated that they're now oligapolizing the market, and will slowly start to increase
their insurance rates and profits once again.
(Socialist or not..the WSWS writers continue to state that which NEEDS to be hammered home)
"The vast wealth of the financial oligarchy, expressed in their ownership of massive corporations, must
be seized and expropriated, while the complex technologies, supply chains, and advanced transportation
systems must be integrated in an organized, planned manner to harness the anarchic force of the world
economy and eliminate material scarcity.
Amazon is a prime example. Its supply lines and delivery systems could distribute goods across the world,
bringing water, food, and medicine from each producer according to his or her ability, to each consumer
according to his or her need.
The massively sophisticated computational power used by the technology companies to censor and blacklist
political opposition could instead be used for logistical analysis to conduct rescue and rebuilding missions
in disaster zones like Houston and Puerto Rico. Drones used in the battlefield could be scrapped and rebuilt
to distribute supplies for building schools, museums, libraries, and theaters, and for making Internet
service available at no cost for the entire world.
The ruling class and all of the institutions of the political establishment stand inexorably in the way of
efforts to expropriate their wealth. What is required is to mobilize the working class in a political
struggle against the state and the socio-economic system on which it is based, through the fight for
socialism.
Eric London "
Advanced technology is helpful but not essential for a humane and just society. Its what we believe and
feel that matters. FWIW, I like socialism on a national/international level and individual accountability
on a personal level.
While general medical care is single payer in Canada, dental services are not. For major work on teeth, it
is cheaper to fly to Mexico. The downside is for Mexicans -- such practices will drive the costs up in Mexico.
Mark, today's posting provided is a nice change of pace to a topic of local impact (for me at least). UGC
presented a good overview peppered with supporting data.
In an earlier career incarnation, I worked as a systems analyst involved with development of online
systems for state social services. Data showed that our systems were able to administer a comprehensive
health care program for social services recipients for about 3-4% of the cost of services. Private medical
insurance providers required approximately 20% of the cost of services to provide similar services. Yet,
private providers were supposedly driven by invisible market forces to maximum efficiency. BS. In fact, they
are driven by greed and they found it much easier to maximize profits by colluding with politicians and
health care providers. That is the trouble with free markets – its just so damn easy to cheat and cheaters
are never in short supply.
One more thing, prescription drugs costs may exceed $600 billion in the US by 2021:
That would be nearly $2,000 per year for every American!
If a tiny fraction of that amount were spent on prevention, education, improved diets and other similar
initiatives, the population ought to be healthier and richer. But, greed overpowers the public good every
time. The US health care system is a criminal enterprise in my opinion. The good that it does is grossly
outweighed by greed and exploitation of human suffering.
I agree with that. Plus, it seems like they have an entire staff dedicated to giving their "customer" the
run around. A friend of mine had to deal with several different departments regarding his healthcare
bill. The billing office told him that they only deal with billing questions, and that for explanations
for the bill, he should call the doctor's office. The doctor's office told him to call the hospital,
since that's where the service took place. The hospital told him to call his primary doctor, who sent him
there, and his primary doctor referred him back to the specialist, where he was referred back to the
billing department, which promptly told him that they're closing for the day, since he spent 6 hours
being transferred from one department to the next.
I find it terribly silly that we should even consider med student's debt as an excuse. First, American
doctors are the best paid professionals in the country. Internists make a median 190 thousand a year, and
they are among the worst paid specialties. I cannot possibly see the problem with paying your income for 5
years, knowing that you get access to a caste that will allow you make good money into your eighties.
Second, the debt is not that high as you claim. Harvard Medical School tuition is 64 thousand. You can rent
across the street with 20 thousand a year – I currently live there.
Third, med students know all this. The reason why they borrow far more is because they know they can
afford it. I went to med school somewhere in a developing world. We shared toilets in the dorm. As a matter
of fact, most under-30s in Boston live in shared accommodation. The outliers? Med students. Even the lowly
Tufts and BU students that I met own cars and live by themselves, mainly in new buildings across the street
from their hospitals.
Every time I go to the doctors, I am thinking how I am going to sue their asses if they make a mistake.
It's not an excuse. It's a bill. When you rent an apartment, did you know that most landlords also factor
in the property tax when figuring out what your rent payment should be? Similarly, the interest payments
on the doctoral students' loans are passed off to the consumer, and that is yet another reason why
Healthcare is so expensive. That's why I think that medical school should be free for those students who
promise to charge their patients no more than x amount of money.
Interesting article. Looks like the rot in the US is terminal. But Canada and its "socialized" medicine is
not far behind. Operating an emergency ward with only one doctor doing the rounds at the rest of the
hospital during the night is absurd. But that is what major Canadian hospitals do. Don't bother going to
emergency at 2 am unless you are literally dying. Wait until 7 am when the day day crew arrives and you can
actually receive treatment.
The problem in Canada, as in the USA, is overpaid doctors and not enough of them (because they are
overpaid). Instead of paying a doctor $300,000 per year or more, the system needs to have 3 or more doctors
earning $100,000 per year. Then there is no excuse about being overworked and "requiring" a high
compensation. Big incomes attract crooks and not talent. If you want to be a doctor then you should do 5
years of low income work abroad or at home. That would weed out a lot of the $$$ in the eyeballs leeches. A
nasty side effect of having overpaid doctors and living adjacent to the US, is that they act like a mafia
and extort the government by threatening to leave to the USA. I say that the Canadian provinces should make
all medical students sign binding contracts to pay the cost difference between their Canadian medical
education and the equivalent in the USA if they decide to run off to America.
At the undergraduate level, the physics courses with the highest enrollment are aimed at streams going
into medicine. There are hordes of money maker wannabes trying to make it big in medicine. But they are all
nearly weeded out and never graduate from medical school. So the system maintains the fake doctor shortage
and racket level salaries. On top of this, hospitals pay a 300% markup for basic supplies (gauze, syringes,
etc). It is actually possible for private individuals to pay the nominal price so this is not just a theory.
Clearly, there is no effort to control costs by hospital administrations since basic economics would imply
that hospitals would pay less than individuals for these items due to the volume of sales involved. At the
end of the day North American public medicine is a non-market bloating itself into oblivion since the
taxpayer will always pay whatever is desired. That is, the spineless politicians will never crack the whip.
This is part of the problem in Canada. One way to help deal with it in my view, beyond simply cutting
doctors' fees (which any government with the political will to do so can do) is to simply make it easier
for International Medical Graduates to get licensed in Canada. Canada has legions of immigrants (and
could have pretty much however many more it likes) with full medical qualifications who would be thrilled
to work for much less than the current pay rates. It's a scandal how many qualified doctors we have in
Canada driving taxis rather than practicing medicine. If we just took advantage of the human resources we
already have, we could easily say to doctors who threaten to leave for the US, "Fine, go. We've got 10
guys from India lined up to do your job." This isn't to say that doctors shouldn't be very well-paid.
Anyone who has ever known someone in med school knows it's hell. But doctors would be very well-paid at
half the rates they're getting now.
Another part of the problem is an over-reliance on hospitals. There
are a lot of people in the hospitals more in "holding" than anything else, because there's no space in
the proper facilities for them (The book "Chronic Condition" talks about this). The problem with this is
that the cost per day to keep someone in the hospital is much higher than in other kinds of facilities.
This is an entirely unnecessary loss.
For all that though, the Canadian system is leaps and bounds better than the American. We spend a
vastly smaller percentage of our GDP on health care, and in return achieve higher health outcomes, as
measured by the WHO. If we were willing to spend the kind of money the Americans do on health care, we
could have patients sleeping in golden beds even with the structural flaws of our current system. That's
worth constantly remembering, because some of the proposals for health reform floating around now lean in
the direction of privatization, and we've seen where that road leads.
Before he retired from politics, Keith Martin was my MLA, and he was also a qualified MD. He used to
rail against the convoluted process for certification in medicine in Canada, while others complained
that we were subject to an influx of doctor-immigrants from India because Canada required less time
spent in medical school than India does. I never checked the veracity of that, although we do have
quite a few Indian doctors. My own doctor – in the military, and still now since he is in private
practice – is a South African, and he explained that he had gone in for the military (although he was
always a civilian, some military doctors are military members as well but most are not) because the
hoop-jumping process to be certified for private practice in Canada with foreign qualifications was
just too onerous.
Unsurprisingly, I completely agree on the subject of privatization, because it
always leads to an emphasis on profit and cost-cutting. I don't know why some people can't see that.
Thanks very much UCG, for your article. Very interesting reading for us Australians as the Federal
Government eventually wants to shove us kicking and screaming into a US-style privatized healthcare
insurance model.
Funnily enough I'm currently considering changing my private health insurer. I'm with Medibank Private at
present but considering maybe going with a smaller non-profit health fund like Australian Unity or Phoenix
Health Fund.
I was just about to post along the lines of "I don't know if Jen has experienced this in Australia but
here in the UK ." so I'll finish the thought. In the UK, successive governments, not just Conservative
ones, have been trying to dismantle the NHS and move us to the American system. It is pure ideology – no
amount of the very abundant evidence of the inefficiencies of the US system, its waste etc makes any dint
in the enthusiasm of those pressing for change.
Thank you Jen! My advice: don't let the Government cajole you into wasting your money on Corporate Greed.
Share the article with your fellow Australians, if you must, but don't let our wasteful system be
replicated. Interestingly enough, one of my friends, Lytburger, send me a meme right after Ukraine
adopted America's Healthcare System, it said: "ISIS refused to take responsibility for Ukraine's
Healthcare Reform!" I'd be happy to provide other data or answer questions about the Healthcare System
here.
As for insurance, I'm not sure if Australia has the in-network and out-of-network rules. Does it?
Whatever insurance you get, make sure that it has good coverage. If you own a home in the US, and you end
up in a hospital's emergency room that's not covered by your insurance, the hospital can take your house
under certain circumstances. Ironically, even the Government cannot. All of my real property is in
various Trust Accounts, just in case, and I make sure that I have insurance where all major hospitals are
in-network and that's the best I can do.
This is s very interesting insight into healthcare in the USA. The cost is shocking.
I live in the UK and the healthcare system is paid for from taxation.
When it was established over 70 years ago the health service would be available to all and financed entirely from taxation, which meant that people
paid into it according to their means.
It was the best thing in my view that government has ever done.
Good healthcare should be available to all and not dependent on peoples ability to pay. However there always a private healthcare system that ran alongside it
And over the years it had been unpicked as successive governments have tried to privatize it. Claiming
they will save the taxpayer money
– opticians and dentistry have become part private after 18 if you are employed.
Which many people do not mind.
-Elderly care was also privatised as it's the most expensive
-care for the disabled also is a issue for local councils
-Mental health became care in the community – society's problem!
Privatisation has meant profits for businesses, poor services to vulnerable groups.
And yet still more and more taxation is needed for the NHS!
The issue of more money was even part of the Brexit debate as it was stated that leaving the EU would mean
more money for the NHS which people are proud of.
There was a quote I was thinking of using in the lead-in, but decided in the end not to since I didn't
want to have too many and it might have become confusing. It related that you would get the best medical
care of your lifetime – after you died, when they were rushing to save your organs, for transplant.
Obviously this would not be true if you were not an organ donor (at least in this country) or died as the
result of general wasting away so that you had nothing left which would be particularly coveted. But this
is a major issue in medicine in some countries and there have been various lurid tales of bodies being
robbed of their organs without family permission, bodies of Ukrainian soldiers harvested of their organs
and rackets in third-world countries where the poor or helpless are robbed of organs while they are
alive. From my standpoint, since I haven't done much research on it, I have seen little proof of any of
them despite plenty of allegation, but it is easy to understand that traffic in organs to those who will
pay anything to live a little longer would be tremendously profitable, and the potential for
disproportionate profit seldom fails to draw the unscrupulous.
As I alluded in the lead-in, Canada has
what is sometimes described as 'socialized medicine' and alternatively as 'two-tier healthcare' although
I have never seen any real substantiation for the latter charge. My mom had an operation for colon cancer
some time back, and she paid nothing for the hospitalization or the operation. My father-in-law is
scheduled for the same operation as soon as he gets his blood-sugar low enough, and he already had one
for a hernia and removal of internal scar tissue from an old injury – again, we paid nothing. He had a
nurse come here for a couple of months, once a week, to change his dressing (because the incision would
was very slow to heal because he is diabetic – nothing. That's all great, from my point of view, and I've
paid into it all my life without ever using it because I was covered by the government under federal
guidelines while I served in the military, although I was a cheap patient because I never had to be
hospitalized for anything and was almost never even sick enough not to come to work. But the great
drawback to it, as I said, is the backlog which might mean you have to wait too long for an operation.
And in my small practical experience – the two cases I have just mentioned – both were scheduled for
surgery within a month of diagnosis. So perhaps the long wait is for particular operations such as heart
or brain surgery.
Thank you very much for a very interesting article UCG! Quite the horror story. I've heard quite a few about
the US over the years from people I know too. I think one of the BBC's former America correspondent gave an
interview to the Beeb as he was leaving America a few years back (MAtt Frei?) and was asked what were the
best and worst things about living there. The worst was certainly healthcare.
I've also read that
healthcare costs for the self-employed, independents, freelancers can also be crushing in the land of the
free where everyone can become rich. Has this changed? I would have thought that those were the ideal
Americans, making it off their own back, but apparently not.
There's also another issue that is not addressed: an ageing population. This is a very current theme and
it is now not at all unusual for people to live another 30 odd years after retirement. Now how on earth will
such people manage their healthcare for such a period? Will they have to hock absolutely everything they
have? America is already at war with itself (hence the utmost need to for
foreign
enemies), but
nothing is getting done. Just more of the same. Meanwhile the Brits are trying to copy the US through
stealth privatization of their health system. It might work as well as privatizing its rail service
Thanks for an interesting post, UCG. Hopefully this will stimulate some ideas on how to fix the American
healthcare system, which seems to be badly broken.
Broken for us but working perfectly for Big Pharma and insurance companies. That is a fundamental reason
why it will be extremely difficult to "fix" because it ain't broken as a money making machine.
With health care in general, there's a bit of a trade-off. The most cost-efficient systems, like the system
in Sweden for example, are fairly regimented and don't leave much room for individual choice (unless someone
pays out of pocket for treatment completely outside the public system). On the other hand, systems that give
people a little more choice, like the system in Germany, tend to be a little on the pricey side. I think,
given American political culture, something along the lines of the German model is much more likely to
attract widespread public support. In any case, it's still cheaper than the American system, and achieves
some of the best results in the world.
https://en.wikipedia.org/wiki/Healthcare_in_Germany
Quite different from my expectation of spartan if not rudimentary medical care and overworked staff in
a small Russian town. The blog on schools was interesting as well. Given where Russia was in the 90's
compared to now, it is easy to understand the strong popular support for the government and Putin in
particular.
Off topic but just saw a 2-3 minute piece on CBS news (a very long story for an American
national news show) about a Russian woman (former Playboy "model') who is challenging Putin. The
reporter assured us the if she became too popular, Putin would never allow her to win. The last time
Russia was allowed to protest, according to the reported was back in 2011 where the masses were
demanding change. The implication being that a subsequent crackdown has suppressed further protest.
The piece showed her speaking to a group (the camera view was such that is was impossible to
determine the audience size but it had to be at least 10 and possibly up to 30 people). The reporter
also speculated that the woman coud be a Kremlin plant to create a fake opposition. Just a mishmash of
a story all in all.
Speaking as someone who has been hospitalized 3 times in Russia and still live
to talk about, I have no complaints.
In the twilight years of the USSR everything was deficit, including medicine, and the hospitals were
often dilapidated, understaffed and lacking modern equipment. It was socialized medicine, of course, but you
only got the basics for "free". They would not let you die, but if you wanted any "extras", you had to pay
or provide "gifts" to the staff. The doctors were and still are good, but were grossly underpaid.
I was first in hospital here, in isolation because I had diphtheria, in 1993. They saved me. I thought my
number was up. When I was recovering, a nurse asked me when my wife would visit me.
"I have no wife."
"Your friends, then?"
"No friends. I only arrived here 3 weeks ago."
"You're going to be hungry!"
Our first child was born in 1999. The maternity wing of Moscow Hospital №1, opened 1837, was nightmarish.
I paid the anaesthetist so that he could ensure that my wife did not suffer during her labour: it was a
long, slow painful birth.
Our last child was born in 2008: brand new hospital; my wife had her own room; everything state-of
the-art. I paid nothing. My wife came out healthy with a healthy baby. I gave the obstetrician a "present"
after delivery.
A bribe? Not in my opinion: just a token of gratitude for a job well done.
I broke my left collarbone at the dacha that same year. I was in a village/small town (Ruza) hospital. It
was only 2-years old. There were problems because I have broken both collarbones before. Anyway, the
orthopaedic surgeon did a good job, and I didn't pay anything: emergency treatment is free for British
citizens, likewise Russians in the UK. A remnant of when the UK and the USSR were glorious allies against
the Beast.
I have also had varicose veins removed. Only 2 days in hospital. A job well done. I gave the surgeon a
present. He didn't ask me for one, but I thought it was right that I do so.
There have been great improvements in treatment and medical technology here. And the doctors and nursing
staff are well trained and competent.
Not perfect -- nothing is -- but more than satisfactory.
Yes, you do hear horror stories, as you do about the British National health Service, but all in all,
satisfactory.
And there is a private health system now financed by private insurance.
And I have had dental treatment here "on the state": no complaints -- and "free", paid by taxation.
An old Russian colleague of mine has lived in Germany many years now, but he comes back to Moscow to see
an orthodontist.
"They are just as good as in Germany, sometimes have even trained there, and much, much cheaper", he
says.
PS I paid the anaesthetist so he could get the best stuff to help a woman in labour and was unavailable
on the state health service. I forget what it was called now: some German manufactured stuff, I suppose.
My wife said it was the norm in Romania to provide small gifts to bureaucrats – too small to be
considered a bribe but a necessary gesture of appreciation. Its not entirely different from the custom
of bringing a small gift when visiting friends (bottle of wine, flowers, box of chocolate, etc.).
Very much so; I'm sure I mentioned before the controversy surrounding my marriage in Russia; the
waiting period that must follow an application to marry is 30 days (I guess this is a period during
which anyone opposing the marriage may make their case), while a tourist visa is also for a maximum
of 30 days. Therefore, I could not legally remain in Russia long enough to get married. Sveta was
very matter-of-fact about it; we would just, she said, announce that she was pregnant, which is one
of the exceptional conditions which will override the waiting period.
I said she would never get
a doctor to sign a certificate that she was pregnant if she was not. Within a week she had her
choice of three. We gave the doctor who furnished the certificate some flowers and a box of
chocolates. I never considered it a bribe, and still do not, and the gift followed the act. We
would have gotten the certificate anyway.
I notice that Russians typically take such a gift with them whenever they visit friends;
Ukrainians do, too. They never arrive empty-handed, and it seems much more a ritualized courtesy.
It seem odds to me how Russia or Romania can be stifling bureaucratic (as ME can attest) yet
rules will often be bent with hardly a blink to facilitate a reasonable request.
The healthcare system in a country probably reflects the dominant elements in said country's culture. Our
family's longtime GP was a buffoon. In my interactions with him his enthusiastic "hands-on" gung-ho approach
caused several problems, not least when I visited him to get a "line" certifying I was unfit for work a week
after a total hip replacement operation (he insisted on examining the wound and re-dressing it with a
dressing whose adhesive I had been tested for in hospital and deemed allergic to it; fun and games, anxiety
and discomfort ).
Nevertheless he made an immediate decision to admit a close relative of mine for surgery on the basis of
his examination of her.
Contracted plan: An agreement between an insurer and a physician stating the physician
agrees to accept a specific dollar amount for each service, regardless of what the physician actually charges for the service.
Allowable: The contracted amount the physician has agreed to accept as complete payment for a service. The allowable
is made up of the portion the insurance will pay and the portion the patient must pay.
Write-off: The difference between the physician's charge and the allowable, which may not be collected from either
the insurance plan or the patient.
Accepting assignment: A physician who accepts assignment agrees to the insurance plan's allowable and write-off
amounts. Some people equate accepting assignment with being a participating physician, but a physician can participate in Medicare
and not accept assignment.
In-network: This originally meant the physician was contracted with a preferred provider organization (PPO),
but now often means a physician is contracted with any plan. This most often comes up when a patient is referred to an out-of-network
provider for services, or when a patient undergoes a surgery or procedure in a hospital that is in-network, but the anesthesiologist,
radiologist, pathologist, intensivist (critical care), hospitalist, emergency room doctor, or neonatologist is not.
"... The Centers for Disease Control and Prevention (CDC) is not billing patients for coronavirus testing, according to Business Insider . "But there are other charges you might have to pay, depending on your insurance plan, or lack thereof," Business Insider noted. "A hospital stay in itself could be costly and you would likely have to pay for tests for other viruses or conditions." ..."
"... Congress needs to immediately pass a bill appropriating funding to cover 100% of the cost of all coronavirus testing & care within the United States. We will not have a chance at containing it otherwise. @tedlieu - as my rep, can you please ensure this is brought up? ..."
"... In the case of the Wucinskis, Kliff reported that "the ambulance company that transported [them] charged the family $2,598 for taking them to the hospital." ..."
"... Last week, the Miami Herald reported that Osmel Martinez Azcue "received a notice from his insurance company about a claim for $3,270" after he visited a local hospital fearing that he contracted coronavirus during a work trip to China. ..."
"... Did anyone expect the unconscionable greed of capitalism to cease when a public health crisis emerges? This is just testing for the virus, wait until a vaccine has been developed so expensive that the majority of the US populace can not afford it at all and people are dropping like flies. Wall Street, never-the-less, will continue to have its heydays ..."
"... The very idea that the defense and "Homeland" security budgets are bloated and additional funding approved year after year but the citizens of this country are not afforded 100% health coverage In a time of global health crisis that could become a pandemic. ..."
"Huge surprise medical bills [are] going to make sure people with symptoms don't get tested. That is bad for everyone." by
Jake Johnson, staff writer Public health
advocates, experts, and others are demanding that the federal government cover coronavirus testing and all related costs after several
reports detailed how Americans in recent weeks have been saddled with exorbitant bills following medical evaluations.
Sarah Kliff of the New York Times
reported Saturday
that Pennsylvania native Frank Wucinski "found a pile of medical bills" totaling $3,918 waiting for him and his three-year-old daughter
after they were released from government-mandated quarantine at Marine Corps Air Station in Miramar, California.
"My question is why are we being charged for these stays, if they were mandatory and we had no choice in the matter?" asked Wucinski,
who was evacuated by the U.S. government last month from Wuhan, China, the epicenter of the coronavirus outbreak.
"I assumed it was all being paid for," Wucinski told the Times . "We didn't have a choice. When the bills showed up, it was just
a pit in my stomach, like, 'How do I pay for this?'"
The Centers for Disease Control and Prevention (CDC) is not billing patients for coronavirus testing,
according
to Business Insider . "But there are other charges you might have to pay, depending on your insurance plan, or lack thereof,"
Business Insider noted. "A hospital stay in itself could be costly and you would likely have to pay for tests for other viruses or
conditions."
Lawrence Gostin, a professor of global health law at Georgetown University, told the Times that
"the most important rule of public health is to gain the cooperation of the population."
"There are legal, moral, and public health reasons not to charge the patients,"
Gostin said.
Congress needs to immediately pass a bill appropriating funding to cover 100% of the cost of all coronavirus testing & care
within the United States. We will not have a chance at containing it otherwise.
@tedlieu - as my rep, can you please ensure this
is brought up?
In the case of the Wucinskis, Kliff reported that "the ambulance company that transported [them] charged the family $2,598
for taking them to the hospital."
"An additional $90 in charges came from radiologists who read the patients' X-ray scans and do not work for the hospital," Kliff
noted.
The CDC declined to respond when Kliff asked whether the federal government would cover the costs for patients like the Wucinskis.
The Intercept 's Robert Mackey
wrote
last Friday that the Wucinskis' situation spotlights "how the American government's response to a public health emergency, like trying
to contain a potential coronavirus epidemic, could be handicapped by relying on a system built around private hospitals and for-profit
health insurance providers."
We should be doing everything we can to encourage people with
#COVIDー19 symptoms to come forward.
Huge surprise medical bills is going to make sure people with symptoms don't get tested. That is bad for everyone, regardless
of if you are insured. https://t.co/KOUKTSFVzD
Play this tape to the end and you find people not going to the hospital even if they're really sick. The federal government
needs to announce that they'll pay for all of these bills https://t.co/HfyBFBXhja
Last week, the Miami Herald reported
that Osmel Martinez Azcue "received a notice from his insurance company about a claim for $3,270" after he visited a local hospital
fearing that he contracted coronavirus during a work trip to China.
"He went to Jackson Memorial Hospital, where he said he was placed in a closed-off room," according to the Herald . "Nurses
in protective white suits sprayed some kind of disinfectant smoke under the door before entering, Azcue said. Then hospital staff
members told him he'd need a CT scan to screen for coronavirus, but Azcue said he asked for a flu test first."
Azcue tested positive for the flu and was discharged. "Azcue's experience shows the potential cost of testing for a disease
that epidemiologists fear may develop into a public health crisis in the U.S.," the Herald noted.
Sen. Bernie Sanders (I-Vt.), a 2020 Democratic presidential candidate, highlighted Azcue's case in a tweet last Friday.
"The coronavirus reminds us that we are all in this together," Sanders wrote. "We cannot allow Americans to skip doctor's visits
over outrageous bills. Everyone should get the medical care they need without opening their wallet -- as a matter of justice and
public health."
Last week, as Common Dreams
reported , Sanders argued that the coronavirus outbreak demonstrates the urgent need for Medicare for All.
The coronavirus reminds us that we are all in this together. We cannot allow Americans to skip doctor's visits over outrageous
bills.
Everyone should get the medical care they need without opening their wallet -- as a matter of justice and public health.
https://t.co/c4WQMDESHU
The number of confirmed coronavirus cases in the U.S.
surged by more than two
dozen over the weekend, bringing the total to 89 as the Trump administration continues to
publicly downplay the severity of the outbreak.
Dr. Matt McCarthy, a staff physician at NewYork–Presbyterian Hospital,
said
in an appearance on CNBC 's "Squawk Box" Monday morning that testing for the coronavirus is still not widely available.
"Before I came here this morning, I was in the emergency room seeing patients," McCarthy said. "I still do not have a rapid
diagnostic test available to me."
"I'm here to tell you, right now, at one of the busiest hospitals in the country, I don't have it at my finger tips," added
McCarthy. "I still have to make my case, plead to test people. This is not good. We know that there are 88 cases in the United
States. There are going to be hundreds by middle of week. There's going to be thousands by next week. And this is a testing issue."
Our work is licensed under a Creative Commons Attribution-Share Alike 3.0 License. Feel free to republish and share widely.
Did anyone expect the unconscionable greed of capitalism to cease when a public health crisis emerges? This is just testing
for the virus, wait until a vaccine has been developed so expensive that the majority of the US populace can not afford it at
all and people are dropping like flies. Wall Street, never-the-less, will continue to have its heydays
A wall street bank or private predator may own your emergency room. A surprise bill may await your emergency treatment above
insurance payments or in some instances all of the bill.
An effort was made recently in congress to stop surprise billings but enough dems joined repubs to kill it. More important
to keep campaign dollars flowing than keep people alive.
fernSmerl 12h I know emergency rooms are being purchased by organizations like Tenet (because they are some of
the most expensive levels of care) and M.D.s provided by large agencies. I'm not as up on this as I should be but a friend of
mine tells me that some of this is illegal. I have received bills that were later discharged by challenge. This is worth investigating
further. Atlasoldie 11h Hmmmm A virus that
overwhelmingly kills the elderly and/or those with pre-exisitng conditions.
Sounds like a medical insurance companies wet dream. As well as .gov social security/medicare wet dream.
The very idea that the defense and "Homeland" security budgets are bloated and additional funding approved year after year
but the citizens of this country are not afforded 100% health coverage In a time of global health crisis that could become a pandemic.
And as has been stated, the unconscionable idea suggested that a possible vaccine (a long way away or perhaps not developed at
all) might not be affordable to the workers who pay the taxes that fund the government? That's insane.
Another example of "American Exceptionalism." China doesn't charge its coronavirus patients, neither does South Korea. I guess
they are simply backward countries.
I own my own home after years of hard work paying it off. It's the only thing of value, besides my old truck, that I have.
If I get the virus, I will stay home and try to treat it the best I can. I can't afford to go to the hospital and pay thousands in
medical bills, with the chance that they'll come after my possessions. America, the land of the _______. Fill in the blank. (Hint:
it's no longer free).
There are other ways to protect your home. Homesteading or living trust. I'm not good at this but I know there are ways to
do it. Hopefully, it would never come to that but outcomes are not certain even with treatment in this case.
As someone
who lost a mother at 5 years old I can sympathize with your grief in losing a daughter-in-law and especially seeing her four children
orphaned. However, I think you miss the point here: This is about we becoming a society invested in each others welfare and not a
company town that commodifies everything including the health and well being of us all.
As a revision it is better but flawed. It is a cost containment bill based on the same research as the republican plan with global
budgets and block grants.
Edited: I encourage you to read this: -ttps://www.rand.org/blog/2018/10/misconceptions-about-medicare-for-all.html Giovanna-Lepore10h oldie:
Part D
Higher education is not free but they do need to become free for the students and payed by us as a society.
Part D is a scam, a Republican scam also supported by corporate democrats because of its profit motive and its privatization
Medicare only covers 80% and does not cover eye and dental care and older folks especially need these services. Medicaid helps but there are limits and one cannot necessarily use it where one needs to go.
Expanded, Improved Medicare For All is a vast improvement. because it covers everyone in one big pool and, therefore, much more dignified
than the rob Paul to pay peter system we have.
Social Security too can be improved. Why should it simply be based on the income of the person which means that a person working
in a low paying job in a capitalist system gone wild with greed will often work until they die.
Pell grants can be eliminated when we have what the French have: publicly supported education for everyone.
The demise of unions certainly did not help but it was part of the long strategy of the Right to privatize everything to the enrichment
of the few.
The overall competence that Canada is handling this outbreak, compared to the USA, is stark. First world (Canada) versus third-world
(USA). Testing is practically available for free, to any suspect person, sick or not, as Toronto alone can run 1000 tests a day and
have results in 4 hours. That is far more than all the US's capacity for 330 million people.
I wonder how long before Canada closes its borders to USAns? Me and my wife (both in a vulnerable age/medical group) should seriously
consider fleeing to my brother's place in Toronto as the first announced cases in Pittsburgh are probably only days away. What about
our poor cat though? We could try to smuggle her across the border, but she is a loud and talkative kitty
Don't want to discourage anyone from any protective measures – but the
"low down" from my veggie store today was that a lot of health professionals
shop there and they think it's being hyped by media. Did get this from my NJ Sen. Menendez –
Center for Disease and Control and Prevention (CDC)
There is currently no vaccine to prevent coronavirus disease 2019 (COVID-19). The best way to prevent illness is to avoid being
exposed to this virus. However, everyday preventive actions can help prevent the spread of respiratory diseases:
Wash your hands often
Avoid close contact with people who are sick.
Avoid touching your eyes, nose, and mouth.
Stay home when you are sick.
Cover your cough or sneeze with a tissue, then throw the tissue in the trash.
For more information : htps://www.cdc.gov/coronavirus/2019-ncov/about/prevention-treatment.html
How it spreads : The virus is thought to spread mainly from person-to-person. It may be possible that a person can get
COVID-19 by touching a surface or object that has the virus on it and then touching their own mouth, nose, or possibly their
eyes, but this is not thought to be the main way the virus spreads. [Read more.] https://www.cdc.gov/coronavirus/2019-ncov/about/transmission.html )
Symptoms : For confirmed coronavirus disease 2019 (COVID-19) cases, reported illnesses have ranged from mild symptoms to
severe illness and death. Symptoms can include fever, cough, and shortness of breath.
Don't want to discourage anyone from any protective measures – but the
"low down" from my veggie store today was that a lot of health professionals
shop there and they think it's being hyped by media.
I agree it is being hyped by the media to the point of being fear mongering. At the same time it is being ignored by the administration to such an extent that really little almost nothing is being done. At some point the two together will create an even bigger problem.
It is like the old adage: "Just because you are paranoid doesn't mean they aren't out to get you." Each over/under reach in considering the reality of the situation has its own problem, which multiply when combined. Every morning when I wake up I say a little atheistic prayer to myself before I get out of bed: "Another day and for better or
worse...".
Well, two reported here in Florida tonight. One in my county, one in the county next door. And more of the "we already knew, but told you late". One person checked into the hospital on Wednesday. We hear it Monday night.
Both were ignored far a long time it seems, and 84 in particular are being watched (roommates, friends, hospital workers not alerted
for several days, the usual). But no one knows every place they had been since becoming infected.
Oh, and they have tested a handful of people. No worry?
I can't see anyway that this level of incompetency is an accident. Spring break is just starting usually a 100's of thousand tourist
bonanza.
So the question is do they want to kill us, or just keep us in fear?
I think the later. But the end result is a crap shoot. So once again, it is a gamble with our lives.
The business of America is business. Sometimes that can go too far and this is one of those times. Making money from the loss,
distress, harm and suffering of others is perverse beyond belief.
"... If you want proof that private equity is predatory, you need go not further than its concerted efforts to extend and intensify the devastating practice of surprise billing. ..."
"... Physicians' groups, it turns out, can opt out of a contract with insurers even if the hospital has such a contract. The doctors are then free to charge patients, who desperately need care, however much they want. ..."
"... This has made physicians' practices in specialties such as emergency care, neonatal intensive care and anesthesiology attractive takeover targets for private equity firms . ..."
"... Emergency rooms, neonatal intensive care units and anesthesiologists' practices do not operate like an ordinary marketplace. Physicians' practices in these specialties do not need to worry that they will lose patients because their prices are too high. ..."
"... It's not only patients that are victimized by unscrupulous physicians' groups. These doctors' groups are able to coerce health insurance companies into agreeing to pay them very high fees in order to have them in their networks. ..."
If you want proof that
private equity is predatory, you need go not further than its concerted efforts to extend and
intensify the devastating practice of surprise billing.
Bad enough that patients develop
afflictions or have accidents that land them in the hospital. Recovering physically is hard
enough. But to then have the stress and financial damage of large and unexpected bills, which
are exercises in rent extraction, is the sort of thing that creates Madame DeFarges.
Private equity experts Eileen Appelbaum and Rosemary Batt did the sleuthing to document how
private equity has greatly extended and profited from this abuse. What most people do not
realize is the degree to which hospitals have outsourced what most people would assume were
core functions provided by doctors on the hospital's payroll, such as emergency room doctors.
With many large nominally not-for-profit hospital groups run by MBAs out to justify higher pay
packages for themselves, many practice areas are in fact outsourced. Private equity has
hoovered up these groups. They, and not the hospital, provide the personnel for a particular
case, and they make sure to get some out of network practitioners on the team to pad the
bills.
One metric: a Stanford study determined that the odds of getting a surprise bill had
increased from 32% in 2010 to 43% in 2016, and the average amount had risen over that time
period from $220 to $628. A new study in Health Affairs found that this out of network billing
raises health care costs by $40 billion per year .
Physicians' groups, it turns out, can opt out of a contract with insurers even if the
hospital has such a contract. The doctors are then free to charge patients, who desperately
need care, however much they want.
This has made physicians' practices in specialties such as emergency care, neonatal
intensive care and anesthesiology attractive takeover targets for private equity firms
.
Emergency rooms, neonatal intensive care units and anesthesiologists' practices do not
operate like an ordinary marketplace. Physicians' practices in these specialties do not need
to worry that they will lose patients because their prices are too high.
Patients can go to a hospital in their network, but if they have an emergency, have a baby
in the neonatal intensive care unit or have surgery scheduled with an in-network surgeon,
they are stuck with the out-of-network doctors the hospital has outsourced these services to
.
It's not only patients that are victimized by unscrupulous physicians' groups. These
doctors' groups are able to coerce health insurance companies into agreeing to pay them very
high fees in order to have them in their networks.
They do this by threatening to charge high out-of-network bills to the insurers' covered
patients if they don't go along with these demands. High payments to these unethical doctors
raise hospitals' costs and everyone's insurance premiums.
Appelbaum cited Yale economists who'd examined what happened when hospitals outsourced their
emergency room staffing to the two biggest players, EmCare, which has been traded among several
private equity firms and is now owned by KKR and TeamHealth, held by Blackstone:
.after EmCare took over the management of emergency services at hospitals with previously
low out-of-network rates, they raised out-of-network rates by over 81 percentage points. In
addition, the firm raised its charges by 96 percent relative to the charges billed by the
physician groups they succeeded.
The study also described how TeamHealth extorted insurers by threatening them with high
out-of-network charges for "must have" services:
in most instances, several months after going out-of-network, TeamHealth physicians
rejoined the network and received in-network payment rates that were 68 percent higher than
previous in-network rates.
California and the Federal government tried to pass legislation to curb surprise billing. As
we noted, the California bill was yanked suddenly and no one felt compelled to offer an
explanation. The bi-partisan Federal effort also failed.
Early in the summer of 2019, Congress appeared poised to protect consumers from surprise
medical bills and to hold insured patients financially harmless in situations where they were
unable to choose their doctor .
Two solutions, both of which take surprise charges to patients out of the equation, have
been put forward. Employers, patient advocates, and insurance companies favor paying
out-of-network doctors a rate "benchmarked" to rates negotiated with in-network doctors to
hold down health costs. Not surprisingly, this solution is opposed by large physician
staffing companies and specialist physician practices that want to continue to charge prices
higher than the in-network fees. These doctors' practices, some backed by private equity
firms, have been lobbying intensively for a second option that would allow doctors
dissatisfied with a negotiated rate to seek a higher fee via an arbitration process that they
believe will ensure higher physician pay and higher company revenues and profits.
The campaign by Physicians for Fair Coverage, a private equity-backed group lobbying on
behalf of large physician staffing firms, launched a $1.2 million national ad campaign in
July to push for this second approach.8 The lobbying campaign bore fruit. In July, [sponsors
of the House bill] Pallone and Walden accepted an amendment to allow arbitration, but only in
special cases, and it required the arbitrator to use negotiated rates instead of provider
charges when deciding on disputes over payment.9 But the private equity-owned physician
staffing companies were not satisfied. In late July, a mysterious group called Doctor Patient
Unity launched a $28 million ad and lobbying campaign (now up to nearly $54 million) aimed at
keeping any legislation to protect patients from surprise medical bills from passing. In
mid-September, a representative for Doctor Patient Unity finally revealed what many observers
already suspected -- that PE-owned doctor staffing firms Envision Healthcare and TeamHealth
were behind the campaign
Agreement on a joint House and Senate bipartisan bill by Senators Alexander and Murray and
Congressmen Pallone and Walden nearly made it into the omnibus continuing resolution that
passed in December 2019. It was stymied when Massachusetts Congressman Richard Neal, Chair of
the House Ways and Means Committee, offered a last-minute alternative. The Neal bill protects
consumers from surprise medical bills but requires disputes between providers and insurance
companies to be resolved through arbitration. This, of course, is what the PE-owned staffing
firms and the doctors' practices they own lobbied for. Lack of support from the Democratic
leadership in the Senate and the House delayed passage of the legislation. In his September
2019 fundraising report, Neal reported receipt of $29,000 from Blackstone, owner of
TeamHealth.
The entire article is
very much worth reading , since it offers more detail on how the private equity firms
tightened their grip on these chokepoints. And the threat of legal curbs has had an impact. As
the piece also explains, the value of the debt on Envision, the parent of EmCare, and
TeamHealth both fell into junk terrain and rebounded a bit when the bills were sidelined for
2019, but remains distressed:
Appelbaum and Batt are pessimistic that anything will get done in 2020:
In the current legislative session, Congress is again working to pass legislation to
protect patients from surprise medical bills. But the disagreements in Congress remain
unresolved Chances of a compromise bill emerging in this session of Congress do not look good
as of this writing (mid-February 2020), and relief for insured patients from unexpected
medical bills does not appear to be on the horizon.
However, bond investors clearly think there's still a risk of legislation with some teeth,
although the earliest possibility is 2021. Keep your fingers crossed.
Where I live the emergency room doctors are contracted out to a private group. This
has been the practice for over a decade. Recently the local hospital got rid of their
dialysis services by selling it to a private company. When a person is sick they don't think
about asking if the provider is in their network. They simply want treatment to help
recover.Another problem is in many areas there isn't a choice. Expensive services can have
only one or no providers. That means you have to go out of you area and probably your
network. I'm on medicare and chose to be on traditional medicare. You aren't locked into a
small network of providers. My supplemental is through my former employer. Unfortunately it's
network plan. Occasionally I have services not paid because they are out of network, even
though medicare covers 80%. The deductible for out of network is so high that I end up with
paying the 20%. I believe there is only one reason for network heart care. It's to increase
profits and has little to do with reducing costs.
I was thinking of Al Capone and his almost untouchable Chicago 'enterprise'. He was
untouchable in Chicago because his racket paid off the judges, prosecutors, aldermen, and
politicians. It took the feds stepping in to shut Capone down.
How many more people will go bankrupt, or avoid going to the doctor or hospital for
fear of bankruptcy because of this PE surprise billing racket? Several state leges are
passing or trying to pass legislation to block surprise billing.
I hope that you've been negotiating your out of network billings! A third or half
off may not be unreasonable. Heck, the hospital only collects about 25% of its total
billings!
This is one reason we need traditional M4A. Traditional Medicare has payment limits
that the provider has to accept if they bill Medicare. (Medicare fraud is a problem, but it
is tracked and prosecuted.)
Maybe I'm missing something, but offhand I don't see how this can even be a thing
under a single-payer health-care system. If someone knows better otherwise, please enlighten
me.
If I've got that much right, could this be another part of the motivation against
M4A?
Of course providers are all worried that compensations will be too meager and
oppressive. For instance if the docs' income expectations go unmet, then they will certainly
buck!
But the "providers," as in the MDs, are not the beneficiaries, or at least not much.
It's the companies that own the practices .which are owned by PE funds.
This reminds me of the TV ad running lately featuring a nice young couple opening
their cable bill and declaring "Its a ransom note!" as if its the height of comedy that we
are living in a kleptocracy where everyone is constantly subject to "your money or your life"
banditry we pretend were left behind in central park muggings of the 1970s.
I have recently had multiple occasions that I needed to write on patient
responsibility forms that out of network and balance billing is refused, followed with
letters citing applicable state laws and CMS contracts barring conduct in my state. It's
insane.
Still I have stacks of collection notices I must beat back and win every time. They only need
to win once to destroy someone. Have we no prisons?
The rapine and dispossession of late-stage American crapitalism (can we finally get
to End Stage?) always exceeds our worst expectations.
Crime-infested swamp of a country.
Dare we hope a movement can coalesce and endure after a decent man in his waning
years is thrust into an historical opportunity to move this train wreck from
disaster?
He's the community organizer Obama never was and the new dealer FDR never quite
was.
In the flatness of our current political terrain, Bernie's grandfatherly menscheism
makes him a moral colossus next to the sniveling careerists and the nefarious old
crassus.
1776, 1860, 1932, 1968. What will we make of this year?
Can you put the rebuttal into your own easily reproducible form? Either a neat page
to staple thoroughly to the bills (copied/printed in needed quantities) or a big rubber stamp
with blanks to fill in if applicable?
Yes, if you can provide it, I would make it a post. Your version with your state's
language and how to find similar language in other states. This is VERY important.
Note I have heard one reader say that their doctors said they wouldn't schedule the
surgery if she made an issue out of out of network MDs, that she needed to go elsewhere. So
those doctors were completely on board with this practice.
Doesn't mean that can't get a judgment against you! Then you spend the rest of your
life trying to avoid having people send money via Paypal or other services direct to your
bank account since they can take it. Or winning the lottery or buying a new car the list is
endless.
As in "Privatize Sovereignty, Socialize Property" by David Cieplay, Blackstone and
its ilk have this very business model. In this case they are buying up emergency room
doctors' practices – with the promise they will make more money – and passing the
cost on to insurance companies (poetic justice) and the state and federal gov. Because we
have no laws against this sort of corporate privateering (heaven forbid congress should
suddenly remember how and why to legislate), all the costs of health care are socialized and
because the PE funds are untouchable they have effectively privatized sovereignty. When we
all realize their useful function in this scam is one big nothing burger, congress will have
to act. It's just another testament to how venal, immoral, lazy and rotten congress is. I can
smell it from here.
Besides PE, it also makes sense that the real estate sector in general would be
opposed to anything that reduces financial burden (particularly anything that would lessen
medical debt) on middle- and lower-middle-income households, because foreclosures and
desperation fire sales would then dry up.
The law protects consumers from surprise medical bills when:
An enrollee goes to an in-network facility such as a hospital, lab or imaging center, but
services are provided by an out-of-network health provider.
An enrollee receives emergency services from a doctor or hospital that is not
contracted with the patient's health plan or medical group.
I've been a relatively healthy individual and so rarely use my insurance. I used it
for the first time in 20 years for a full yearly physical (just because it was "that time",
not for any health problems). The annual full checkup is, supposedly, fully covered, and I
chose a local clinic in my network.
The various clinics involved ended up billing me directly, so far, for over
$3500.00, and that was before the colonoscopy bill which still hasn't arrived. I checked my
Insurance Portal and, sure enough, the supposed covered charges were listed as
"Denied".
So, considering all these costs were supposed to be covered, I took a full day off
work (6 solid hours on various phone calls) to get it straightened out. While going through
all these bills and working through each charge I discovered 1 bill for a clinic appt (a
subsidiary of CVS) that never happened and 1 very high bill for standard blood tests (Quest)
that never happened due to a screwup initiated by the CVS-owned clinic. We'll see what
happens.
But while talking with one of the Insurance Co. reps she told me a classic surprise
billing horror story that happened to her. She gets occasional nosebleeds and one day got a
serious one while on the highway before her exit. A CHP officer pulled up behind her after
she pulled over to take care of the situation and refused to let her continue on without
going to the nearest Emergency Room, so she went.
Her visit lasted 1/2 hour. She was handed a bucket of clean water and a towel. After
cleaning up, she waited around for awhile, gave up waiting, washed the towel out, cleaned the
bucket out and left. She went on to tell me that 30 days later she recieved a bill from the
Emergency Services group at the hospital for $45,000.00. For a towel and a bucket of
water.
It took her two days of unpaid time off to get it straightened out and the bill
removed.
She then told me she's voting for Sanders, too.
So I've learned three lessons from this; 1) even with insurance things go wrong far
too often when it comes to billing issues, and 2) Surprise Billing is far more common than I
was led to believe, and 3) Health Insurance/care in this country is riddled with fraud and
outright criminality.
Hate to tell you, but with a colonoscopy, the exam is covered by Obamacare, but any
snipping of polyps is not, and that can easily run to $1000.
The US Is the only advanced economy where colonoscopies are recommended for everyone
over 50. In other countries, they are recommended only for people in high risk
groups.
If you get an annual ( and it needs to be annual ) fecal occult blood test
(easy and cheap, MD puts gloved finger in you, wipes test panel, and tells you right there),
the results in terms of detection are on par with colonoscopies.
Healthcare I had wondered why the Senate
(Schumer) had backed off on legislation controlling surprise billing. It turns out there is a
House bill also and I am sure they are going back and forth on this. Recently, two bills have
emerged in the House and one from the Senate. Medscape , "House Committees Advance
Bills to Address Surprise Billing."
Of course if Congress's butt was on the line, a solution would have been found quickly and
enacted in 2020. At the end, see which one I would back.
The House Ways and Means Committee bill passed by a voice vote bipartisan bill. It seeks to
establish more use of third-party negotiators ( arbitration) for settling certain disputes
about payment for out-of-network care. This bill has the support of the American Hospital
Association and the American College of Emergency Physicians. The American Medical Association
also praised the committee's reliance on mediation for disputes on bills.
The House Education and Labor Committee advanced a hybrid proposal seeking to use
established prices in local markets to resolve many disputes about out-of-network bills. Key to
this bill is the use of arbitration above a certain cost. Bills greater than $750 or in the
case of air ambulance services $25,000; clinicians and insurers could turn to arbitration for
an independent dispute resolution. House Education and Labor passed this bill in a 32-13 mixed
vote with some Republicans and Democrats opposing and in favor.
The latest Senate Health, Education, Labor and Pensions (HELP) Committee of legislative
proposals also addresses surprise medical billing. The HELP bill called for mandating that
insurers reimburse out-of-network costs on the basis of their own median rates for in-network
providers.
The Education and Labor Committee bill is estimated to save $24 billion, the Senate HELPS
bill is estimated to save $25 billion, and the Ways and Means' bill would save almost $18
billion all over 10 years. It is suggested the greater use of arbitration in the Ways and
Means' bill will result in less savings.
Read on about the private equity involved and providers.
Outside Opponents of Legislation
The
American Hospital Association : "Setting a rate in statute gives insurers few incentives to
develop robust networks with hospitals and physicians, and paying for emergency care at the
median in-network rate would surely underpay for these services and create an incentive for
insurers to avoid paying fair reimbursement for these services. This approach is an obvious
windfall for the insurance industry without any assurance that health plans will pass these
savings on to consumers through lower premiums."
Other physician organizations have joined the fight to make balance billing appropriate; the
American College of Emergency Physicians, Envision Healthcare, US Acute Care Solutions and US
Anesthesia Partners -- gave roughly $1.1 million in 2019 to members of Congress, according to a
Kaiser Health News analysis of Federal Election Commission records.
Doctor Patient Unity
: "We support a federal solution to surprise medical bills that makes insurance companies pay
their fair share and supports patients' right to quality medical care."
"We oppose insurance-industry-backed proposals for government rate setting that will lead to
doctor shortages, hospital closures and loss of access to medical care, particularly in rural
and underserved communities."
Early on in 2019, Doctor Patient Unity spent more than $28 million on ads opposing
legislation without disclosing its staff or its funders. It was later revealed its
largest financial backers are two private equity backed firms Team Health and Envision
Healthcare. Together they own physician practices and staff emergency rooms around the country
according to spokesperson Greg Blair. Blackstone Group owns Team Health and KKR owns Envision
Healthcare
As is typical of political ads being run to influence people, they do not tell the whole
story and omit references to surprise bills. Instead, they warn of "government rate setting"
harming patient care and doctor/patient relationships.
The Direct Providers
ER doctors, anesthesiologists, radiologists and other specialists who typically charge
out-of-network prices are among the highest-compensated practitioners. I have found this to be
true during my hospital visits. Doctors, 3rd party contracting companies, and hospitals
complain Healthcare Insurance Companies have the upper hand due to size and can pay the
increased costs of out-of-network pricing.
The argument by doctors, the 3rd party contracting companies, and hospitals has been made
the healthcare insurance companies control the market and are able to secure better pricing
from providers which is not passed along to the insured. In markets where both
providers and insurers are highly concentrated, insurers have bargaining power to reduce
prices for hospital admissions and visits to certain physician specialists. The Market
Concentration chart for insurers and providers reveals the concentration (concentration chart)
for providers is greater than it is for insurers overall. Furthermore and if we are talking
about ACA policies, additional moneys gained must be used for treatment or the excess beyond 15
and 20% overhead and profit is refundable. It can be said also, when the total cost goes up,
the portion (15 or 20%) of the total price increases in real dollars.
ER doctors, anesthesiologists, radiologists and other specialists who typically charge
out-of-network prices are among the highest-compensated practitioners. I have found this to be
true during my hospital visits. If the insurance company can not convince them to take a lesser
rate, you are stuck will the bill. I have been tempted to ask at the time of need whether they
are all in network and employees of the facility I am visiting that day. Countering the
argument by insurance, doctors, and hospitals complain healthcare insurance companies have the
upper hand due to size and market control and can pay the increased costs of out-of-network
pricing. As shown chart 1, their claims are not precisely true and the market for healthcare
has become less competitive as hospitals and ACOs buy up the competition.
"Providers are more concentrated than insurers in almost 60 percent of US metro
areas . Health plans hold an edge in only 6 percent of local markets. National and state
level studies reveal a steady rise in concentration among specialist physicians, primary care
providers, and hospitals alike. As Brent D. Fulton notes, concentration of
insurers fell slightly from 2010 to 2016, while concentration rose for both specialist
physicians and hospitals. The evidence suggests provider organizations will retain significant
bargaining leverage even after out-of-network billing reform, leaving little scope or incentive
or capability for insurers to push prices down sharply. "
Meanwhile, the naysayers are battling constructive resolution with $millions in countering
ads and intense lobbying of Congress to delay and/or deny resolution of overpriced surprised
billing of patients of which had no choice, many more are still being hit with bills there is
little explanation for except greed. We do need Single Payer. Nough said . . .
Congress has till February 22nd to resolve the deadlock before the current temporary bill
expires. I would take the Education and Labor approach, which is also backed by the House
Energy and Commerce Committee, and the Senate Health Committee. It would set the payment rate
based on the median amount paid for that service in the geographic area with the option of
going to arbitration for some higher-cost bills. It result in greater savings.
steve , February 18, 2020 5:25 pm
We (anesthesiology) are par with everything that our network accepts. I am not a fan
of surprise billing, but I dont think you grasp all of the issues here. Medicare
reimburses at much lower rates than does private insurance in my specialty. If you work
in a place with a high percentage of Medicare (or Medicaid which is worse) like we do,
you cannot come close to earning market salaries. So we, many years ago, ended up working
95th percentile or worse hours (over 70 per week) while earning in the 15th-20th
percentile in income. We lost a lot of staff. The hospital had to make up the difference
so that we could hire and retain people. We were fortunate that our hospital had the
resources to do that.
Up north of us another hospital faced a similar situation, but they didn't have the
resources to subsidize their staff. So they fired a good team and brought in another.
Told them it was OK to not bill in accordance with what the hospital accepted, like the
prior group did. That let the new group earn enough, for a while, to hire and retain
people. Hospital eventually failed anyway and had to be bought out.
I think most of the groups that I know are surprise billing are pretty greedy and
sleazy, so I stay away from them. However, there are other cases where groups are in a
tough situation and pretty desperate. Especially smaller rural hospitals that have
trouble finding staff to begin with.
Thank you for this post. This is an important topic that needs to be discussed.
Again Dr. ZDogg: "Guess what's going to happen to her insurance premiums next year?
They're going to go up by 10%, 15%, 20 percent. And what will happen at employers around
the country who are paying most of the bill? They're going to drop or keep wages flat
(happening today). Healthcare becomes a financial albatross with collusion between
healthcare providers charging a bunch of money and insurance companies paying it, hospitals
overbuilding, overcharging, and doing stuff we don't even need. The results of these money
games are a minority of people getting rich and everybody else's wages staying stagnant. 1
in 5 Americans have collection agencies coming after them for medical bills that are
inflated and unnecessary.
BTW this is the same price inflation dynamic that we observe in body shops and car
insurance companies. Kind of evil symbiosis that develops. So this is a more general
phenomenon than just healthcare.
This is the same spiral of cost inflation that we observe in dealing with repair shops and car insurance companies. They form
symbiosis that prosper by mutual inflation of costs.
Notable quotes:
"... The Insurance company must apply 80% of healthcare insurance premiums to actual care. and 20% to Overhead and Profit. Dr. ZDogg states most of the tests were not needed such as a Pan-Viral test when a rapid-strep swab would do. Dr. ZDogg contends this was a virus and the most one should do is the swab the throat or just wait to see what develops . . . this sounds familiar to me as a patient too. ..."
"... The hypothetical? Lets say at the most, what was done should be about $1000 or $800 to actual care and $200 to Overhead and Profit. Multiple this by 26 and see what it amounts to. In Dr. ZDogg's words: "What if we make the pie bigger and 3% of a bigger pie is more money? What if we actually let people overcharge for procedures they don't need? Then all we have to do next year is raise the premiums to cover the actual medical cost, which is now higher, and then we make a higher amount of profit." That was the untoward side effect of the government policy on this, which, by the way, happens with many policies that are top-down. You can't predict what happens and then it happens. " ..."
Going to her PCP located in Manhattan, a woman complains of a sore throat. Forget the
Manhattan part of this as various versions (surprise billing) of this situation are happening
everywhere. The doctor swabbed the throat, sent it off to the lab, ordered some tests, and then
gave her a prescription for antibiotics. She took her meds and went on vacation feeling
better.
The tests came back negative. She later received a bill for ~$26,000.
The lab was out of network which usually results with insurance only paying a portion of the
bill and the patient the balance unless the insurance negotiates a lesser charge (hospital 3rd
party employees) which they will pay. This is another version of Surprise Billing, not in a
hospital setting, which we have heard so much about, and the patient gets screwed with the
balance of the Surprise Billing.
More Information
The lab was out of network but it was a part of the employer the PCP worked for also.
Usually doctors use the hospital they are affiliated with to run tests or do lab work which are
also in network (today). I suspect more hospitals will relegate lab work to 3rd parties to cut
costs and improve profits.
There was a time when I had catastrophic insurance which only paid 50% of costs. I had
pneumonia and really could not afford to go to my PCP at $150 (then) as I was out of work. My
PCP was not sympathetic and wrote me script to take to the hospital for imaging and another
test. I called the U 0f M hospital and talked to a clerk there about cost. He finally told me
to go to Quest (outside lab) and they would be half the cost in doing imaging, etc. U of M has
some major Overhead to pay for today.
By the way, Blue Cross Blue Shield paid almost all of the bill for this lady with the sore
throat.
Even More Information and a Hypothetical
The Insurance company must apply 80% of healthcare insurance premiums to actual care.
and 20% to Overhead and Profit. Dr. ZDogg states most of the tests were not needed such as a
Pan-Viral test when a rapid-strep swab would do. Dr. ZDogg contends this was a virus and the
most one should do is the swab the throat or just wait to see what develops . . . this sounds
familiar to me as a patient too.
The hypothetical? Lets say at the most, what was done should be about $1000 or $800 to
actual care and $200 to Overhead and Profit. Multiple this by 26 and see what it amounts to. In
Dr. ZDogg's words: "What if we make the pie bigger and 3% of a bigger pie is more money? What
if we actually let people overcharge for procedures they don't need? Then all we have to do
next year is raise the premiums to cover the actual medical cost, which is now higher, and then
we make a higher amount of profit." That was the untoward side effect of the government policy
on this, which, by the way, happens with many policies that are top-down. You can't predict
what happens and then it happens. "
I would like to think doctors, hospitals, and healthcare insurance companies are not prone
to this. Yet we have record of numerous surprise billing instances by hospitals, this one is an
example of one by a doctor. Medicare Advantage plans are over billing CMS for treatments
running totals up to $10 billion per year. And what about Commercial Healthcare Insurance? I
have not heard of insurance pushing back on over charges. Usually, they reject a bill or a
portion of it and the patient pays the balance.
And what Happens as a Result?
Again Dr. ZDogg: "Guess what's going to happen to her insurance premiums next year? They're
going to go up by 10%, 15%, 20 percent. And what will happen at employers around the country
who are paying most of the bill? They're going to drop or keep wages flat (happening today).
Healthcare becomes a financial albatross with collusion between healthcare providers charging a
bunch of money and insurance companies paying it, hospitals overbuilding, overcharging, and
doing stuff we don't even need. The results of these money games are a minority of people
getting rich and everybody else's wages staying stagnant. 1 in 5 Americans have collection
agencies coming after them for medical bills that are inflated and unnecessary.
Dr. ZDogg recommended exposure to sunlight might cure the problem.
The patient; "I made it very clear [to the doctor's office] that I was unhappy about it."
And told them I would report the doctor to New York state's Office of Professional Medical
Conduct. She also reached out to "Bill of the Month," a joint project of NPR and Kaiser Health
News. After a reporter started asking questions about the bill, Blue Cross and Blue Shield of
Minnesota stopped payment on the check it issued and is now investigating.
The bottom line to this is, it should have never got this far or even happen.
Recently it was disclosed Michigan No Fault Accident Coverage was paying an ~289% of
Medicare rates to hospitals and clinics to care for patient injuries suffered from automobile
accidents. No Fault coverage will die in a few years as the new legislation sponsored by
Quicken Loans Dan Gilbert and Michigan Repubs have allowed people to opt out or take lesser
coverage which will now pay hospitals and clinics 220% of Medicare rates. No Fault would not
disclose what it was paying caregivers. Another surprise which should have never happened . .
.
This story is from December 2019 and was in NPR
For Her Head Cold , Insurer Coughed Up $25,865, NPR, Richard Harris.
The solution is to have one network and a single payer. Simple.
run75441 , February 14, 2020 7:49 pm
Chris:
You remind of someone else who insists it is that simple. It is not unless you have
60% of Congress inline. And if you do make the change, look forward to much of the
Senate and the House being replaced as the population likes their Employer sponsored
commercial healthcare insurance in spite of being screwed over by commercial
healthcare, healthcare, and the pols who kiss the industries butt. What you and others
are insisting on as being so simple is not so simple to enact.
davebarnes , February 14, 2020 1:39 pm
I have Kaiser Medicare Advantage and am happy. Colon cancer fix cost me $2500 for surgery + chemo. Perianal abscess cost me $300. Three surgeries.
EMichael , February 14, 2020 2:49 pm
Chris,
The solution is indeed simple. Getting to the solution is a huge task.
Meanwhile, It would be very simple legislation to stop this criminal treatment by providers.
Person has insurance and is treated by someone out of network without giving specific orders to
go out of network, is only liable for the in network charges.
Hard to vote against that, but we all know how many will, and who they are.
The only surprise medical bills I have received is for claims that were denied by my
insurance company. Then the provider does not just demand what they would have received if the
claim had been approved, but the full billed amount, which is generally 2 to 10 times the
insurance amount. Providers should have to charge everyone the same price for the same thing.
Now they have an incentive to order dubious tests or procedures, because if a claim is denied,
they can bill for more money. I assume people without insurance are also billed for the full
amount, and they can least afford it.
I also think that if I call 911 and need emergency assistance, it should be provided by
the city or county, not a private company. That's true if police or fire engines are needed,
and likewise it should be for EMTs or ambulances.
"... If you are on Medicare, do not stay for observation unless you have a Plan G or Plan F. If you are on Plan N Supplemental to Medicare or lower, the plan will NOT pay 100% for Observation. You have to be admitted. You can go anywhere with Medicare for treatment. ..."
"... Medicare Advantage? You had better be in network or have some type of alternative program within your plan. ..."
The idea I have is not to be surprised. I am a careful patient who asks a lot of questions
and also advocate for myself. I have refused treatment when they use drugs which may threaten
my health further (Heparin). I am also not well liked by the bloodsuckers who come in to draw
blood and stab me through the vein for two weeks and destroyed my left arm in the process. Ask
them questions and do not be so willing to accept treatment (if cognizant) until they answer
your questions and then get their name. Take names and dates. It is ok to be a forceful
advocate for yourself. When all is said and done, the bill will come to you alone.
If you are on Medicare, do not stay for observation unless you have a Plan G or Plan F. If
you are on Plan N Supplemental to Medicare or lower, the plan will NOT pay 100% for
Observation. You have to be admitted. You can go anywhere with Medicare for treatment.
Medicare Advantage? You had better be in network or have some type of alternative program
within your plan.
There are good points to this article which is why I C and P-ed it here per their
request.
The cost of healthcare has become a hot topic in American politics in recent years, and with
good reason. A recent survey found that 22 percent
of Americans are losing sleep over healthcare or insurance costs, up from 13 percent just one
year ago.
One aspect in particular has even gained attention from both Congress and the President within
the past two months: surprise medical bills.
Congress has proposed bi-partisan legislation that sets up consumer protections against
surprise billing in certain situations. President Trump also issued an executive order in June
that calls for hospitals to be more transparent upfront about prices for common tests and
procedures, a measure that should go into effect later this year. ( While the House took out
the 10 year exclusivities for Biologic drugs, it ended up in the Budget bill giving exclusivity
for 12 years on new biologics. As I have pointed out repeatedly, risk adjusted R & D costs
are recouped in a median period of 3- 5 years. It is another
give-away to pharma. )
Past the leap, causes and prevention of Surprise Billing.
The cause of surprise
billing
Unexpected medical bills, often outrageously expensive, can catch patients by surprise if
they see a doctor who is not within their insurance network. It's a common issue, with the
Wall Street
Journal reporting that an estimated 51 percent of ambulance rides, 22 percent of ER visits
and 9 percent of elective cases lead to surprise medical costs.
What often happens is that while the hospital or clinic might be considered in-network, a
specific doctor might not be in-network (or vise versa). The legislation proposed by the Senate
includes cost protections for situations such as these, plus scenarios where patients receive
emergency care or follow-up care at an out-of-network facility due to travel restrictions.
While the new legislation and executive action may help patients and their families,
surprise billing will persist in situations outside the purview of these new protections. (
The proposed prevention of surprise billing did not make it through the Senate this time for
reasons I am not aware of today. More later .)
Preventing surprise healthcare
bills
The best way to combat surprise billing is to prevent it whenever possible. This requires
staying up-to-date on your insurance policies and looking at your options when scheduling
appointments.
Know the details of your insurance policy
The first step is understanding your specific insurance policy. Check with your provider for
a list of in-network hospitals, specialists and primary care physicians in your area so you can
know ahead of time where you'll have coverage. If you have an upcoming appointment, it's worth
calling your provider to double-check whether the facility and doctor you're seeing are
in-network and covered.
Your provider may also require prior authorization before an appointment in order to cover
some healthcare services or prescriptions, especially when visiting specialists.
Ask about costs upfront
Whether you're visiting a new primary care physician, seeing a specialist or have a planned
procedure coming up, call ahead to see what out-of-pocket costs you will be responsible for
paying. If you find that the facility or physician is out-of-network, you can request a
referral to a facility or physician that is in-network.
For planned visits, you can also ask about the billing codes for the tests or procedures
you'll be having so that you can confirm that your insurer will cover them. While many standard
preventative procedures like a basic cardiac stress test or mammogram are covered by insurance
policies, more advanced screenings such as a 3D mammogram may be billed under a different code
that is not covered by your insurance.
Make an emergency plan
While it's impossible to predict when emergencies will happen, you can make a plan to help
you prepare. If you know which emergency care providers are covered by your insurance plan, you
can have an idea of where to go. While it requires some research on the front-end, you can save
some stress and a lot of money in the long-run.
Understand your rights
In addition to new federal protections, many states have additional regulations regarding
"balance billing," when patients are billed for out-of-network providers at an in-network
facility. Don't be afraid to negotiate with hospital billing managers or doctors who billed you
when you are balance billed, and keep your insurance company in the loop on the situation.
Knowing your state's specific protections can help you get fees waived or lowered in these
cases.
Combating debt from surprise medical bills
Unfortunately, it's impossible to entirely prevent surprise medical bills -- especially in
the case of emergency services. In an emergency room, you have little to no control over which
physicians you see and what tests are run. You also don't always have time to call ahead to
check prices or request transfers to in-network facilities.
While it might not be possible to prevent some surprise healthcare costs, there are still
steps you can take to combat debt in these cases.
1. Double check itemized medical bills.
Mistakes happen. Sometimes patients are billed for tests, procedures or medications that
they didn't actually receive. Ask for an itemized bill, and ensure that you are only being
charged for services received. If you find a mistake in your bill, talk to the hospital's
billing department and the service provider.
In the case that a procedure or service on your bill should have been covered by your
insurance provider, ask about the specific billing code the hospital used. It's possible that
while the insurance provider covers a basic or general service, the billing code used may not
fall under the billing code your insurance company lists as covered. Talk with both the
hospital billing department and your insurance provider to see what can be done.
2. Avoid using credit cards whenever possible
Credit cards average around a 17 percent interest rate, meaning they are less-than-ideal for
covering high
medical costs . There are medical credit cards out there that offer short and long term
financing plans to cover medical expenses with minimal interest, which is an option for those
who can realistically pay off the debt within the specified time period.
When using a credit card is unavoidable, consider a credit card that offers a long intro
period to help you save on interest charges, such as well known Platinum
Visa Card might offer. If you end up with bills spread across multiple credit cards, a
balance transfer credit
card can also help you eliminate debt and save money on interest charges.
Just keep in mind that for all of these credit options, it's imperative that you can pay off
the debt within the 0% interest offer period. Otherwise, you'll be subject to high interest
rates that can cause even more financial stress.
For larger medical bills or debts, consider a personal loan (which offer lower, fixed
interest rates) to help cover the cost.
3. Protect your credit score
If for any reason you are unable to pay your medical bills on time, it's important to take
steps to protect your credit score. When you go more than 90-180 days without paying a medical
debt, it could become an unpaid collection account, which can show up on your credit report and
negatively affect your score. Luckily, newer credit score models such as the VantageScore 4.0
and FICO Score 9 often reduce the impact of these types of collection accounts.
If you know you'll be unable to pay medical bills, be open and honest with the hospital or
provider. You might be able to set up a plan that better fits your budget. At the very least,
you can explain the situation, pay as much as you can at the moment and potentially prevent
them from writing off your debt as a loss and selling it to a collection agency.
4. Open a savings account for unplanned medical costs
While you can't predict unplanned medical costs, you can prepare for them by saving money
for a rainy day. One option is contributing to a Healthcare Savings Account (HSA), which allows
you to add pre-tax/tax-deductible money into a savings account that you can use for approved
healthcare costs.
You can also set up a savings account with any bank to be used for healthcare costs. While
these accounts may not be tax-exempt, you can often get a better interest rate and avoid
regulations on what medical expenses you can and can't cover with the account.
Even if you only contribute $20 a month, it will add up over time and can help offset costs
to make medical expenses more affordable.
The Bottom Line
While it's promising that both Congress and the President are making strides towards
eliminating surprise medical bills and helping lower overall healthcare costs, sometimes
surprise billing is unavoidable. These tips can help you prevent these charges or combat
excessive debt that can often result from unplanned medical expenses.
davebarnes , January 11, 2020 9:28 pm
Kaiser Medicare Advantage.
Have NEVER has a strange nor bogus charge.
My colon cancer surgery + chemo was $2500 which I consider reasonable.
My 3 surgeries for a perianal abscess (trust me, you don't want one) was a few hundred
bucks.
4.5 miles to the hospital/medical center/pharmacy.
run75441 , January 11, 2020 11:42 pm
That is nice. Your time will come when they will charge more for those operations. You are
there forever and can not come back to Medicare. What do you think is happening with
commercial healthcare today for a majority of the people who have commercial healthcare?
likbez , January 12, 2020 12:09 am
Great post on a very important in the USA topic. Thank you run75441!
I would add the danger of calling ambulance from home in non-critical cases. Taxi to the
hospital is approx. 100 times cheaper and most cases is as effective :-).
In case the case is critical (like a real heart attack) be ready to pay out of network
changes ($5K-$15K) for the ride in states that do not provide protection against surprise
billing. Less then a half of the USA states some minimal (really minimal) protection against
those sharks.
Ambulances in the USA are overtaken by private equity and venture capital firms.criminals.
They are real Mafiosi. Or even worse because they profit of human sufferings. Private equity
sharks circle around and if they smell blood they will devour the victim without any merci. I
sometimes wonder why among around 40K of gun violence victims (39,773 in 2018) in the USA per
year this category is so underrepresented .
The core of the problem is that ambulances and private insurance companies do not agree on
a fair price, so the ambulance service doesn't join the insurance network. That leaves
patients stuck in the middle with out-of-network charges..
One patient got a $3,660 bill for a 4-mile ride. Another was charged $8,460 for a trip
from one hospital that could not handle his case to another that could.
Still another found herself marooned at an out-of-network hospital, where she'd been
taken by ambulance without her consent.
These patients all took ambulances in emergencies and got slammed with unexpected bills.
Public outrage has erupted over surprise medical bills -- generally out-of-network charges
that a patient did not expect or could not control -- prompting 21 states to pass laws
protecting consumers in some situations.
But these laws largely ignore ground ambulance rides, which can leave patients stuck
with hundreds or even thousands of dollars in bills, with few options for recourse, finds a
Kaiser Health News review of 350 consumer complaints in 32 states.
Patients usually choose to go to the doctor, but they are vulnerable when they call 911
-- or get into an ambulance. The dispatcher picks the ambulance crew, which, in turn, often
picks the hospital. Moreover, many ambulances are not summoned by patients. Instead, the
crew arrives at the scene having heard about an accident on a scanner, or because police or
a bystander called 911.
Betsy Imholz, special projects director at the Consumers Union, which has collected over
700 patient stories about surprise medical bills, said at least a quarter concern
ambulances.
As the days go by I become more convinced that the impeachment drama was used to cover up
the passing of the usmca and axing of the venture capital in health care bill and containing
surprise medical billing https://khn.org/news/investors-deep-pocket-push-to-defend-surprise-medical-bills/
FTA "We've started to realize it's not us versus the hospitals or the doctors, it's us versus
the hedge funds," said James Gelfand, senior vice president of health policy at ERIC, a group
that represents large employers.
From the KHN article on surprise billing
"surprise medical bills, which generally arise when an insured individual inadvertently
receives care from an out-of-network provider."
How did "inadvertently" get in there when it is a revenue generation model? Asymmetry of
information is always how profits are made.
I like to invert the model and estimate the outcomes for a lot of these fictions: if
working class people controlled the upward distribution of wealth, how would society be
different?
"... Where is AOC in all this? She was th e prime mover on impeachment, specifically impeachment over a phone call rather than concentration camps and genocide. And now with impeachment she gave Pelosi cover to sell the country out again. I was wondering why many libreral centrists were expreasing admiration for her, a socialist. Maybe they recognized something? ..."
Interesting, to me at least, that the rocket docket timetable of the House impeachment
coincided with the deadline to pass a budget to avoid a(nother) govt shutdown. While all msm
eyes were transfixed by the hyperventilating spectacle, behind the scenes the budget passed
through the Dem House was filled with more tax breaks for the corporations and the .001%,
more money than the admin asked for the MIC, and killed a bill that would end medical
'surprise billing' (another gift to medical PE investors and giant hospital corporations),
basically a whole neolib wish list.
Interesting the two events coincided, and, that Nancy decided not to sent on the articles
to the Senate at this time. What gives? Is she hold on to them for a future time when she'll
need to use them as another distraction for the msm to report on? (no, that could not be the
reason. ;) )
Pointed this out a couple of days ago (Slate and Buzzfeed). Happy that it is not just the
online press pointing out it was Democrats killing this measure, Democrats in leadership
positions. I also like that few, if any, of our media is falling for the kabuki used by Neal
to stick the shiv in. Everyone gets that the 'competing plan' was there strictly to derail a
law that end the hugely profitable but fraudulent price gauging of healthcare by private
equity.
If he keeps this up, walking POS Schumer might make me miss Al D'Amato nah Al and Chuck
are just two different colors of tulle, adding illusion to the political process.
..and they could have just passed it for the good PR and then de-fanged it
administratively, but it looks like they wanted to press the point:
"No, Proles, we're not gonna let you breathe, not a bit."
Where is AOC in all this? She was th e prime mover on impeachment, specifically
impeachment over a phone call rather than concentration camps and genocide. And now with
impeachment she gave Pelosi cover to sell the country out again. I was wondering why many
libreral centrists were expreasing admiration for her, a socialist. Maybe they recognized
something?
"... By 2013, physician staffing firms owned by Blackstone Group and Kohlberg, Kravis Roberts & Co. (KKR) – among the largest PE firms in the country – cornered 30 percent of this market. Since then, private equity ownership of these services has continued to grow. ..."
"... The Stanford study found that the likelihood that a patient admitted to an in-network hospital would face a surprise medical bill because at least one out-of-network doctor cared for them increased from 26.3 percent 2010 to 42.0 percent in 2016. A particularly egregious instance occurred when an assistant surgeon sent a bill for $117,000 to a patient who had surgery for herniated discs in his neck. ..."
"... Commenting on EmCare's relations with hospitals, Benedic Ippolito, a research fellow in public finance and health economics at the American Enterprise Institute, noted, "Right now, EmCare surprise bills patients and hospitals effectively turn a blind eye. ..."
"... A team of Yale University health economists examined the billing practices of EmCare, Envision's physician staffing arm. [xx] They found that when EmCare took over the management of emergency departments, it nearly doubled its charges for caring for patients compared to the charges billed by previous physician groups. These egregious practices have resulted in a Congressional investigation headed by Missouri Senator Claire McCaskill, lawsuits from shareholders, and court actions involving Envision and UnitedHealth Group, the largest U.S. insurer. [xxi] ..."
Surprise medical billing has become a critical issue facing Americans across the country because of purposeful corporate practices
designed to increase profits. As hospitals have outsourced emergency rooms and other specialty care to reduce costs, private investors
have bought up specialty physician practices, rolled them into powerful national corporations, and taken over hospital emergency
services. The result: large out-of-network surprise bills. The hidden actors: Leading private equity firms looking for 'outsized'
returns.
Surprise medical billing made headlines in 2019 as patients with health insurance found themselves liable for hundreds or even thousands
of dollars in unforeseen medical bills. When patients with urgent medical problems go to an emergency room (ER) or are treated by
specialty doctors at a hospital that is in their insurance network, they expect that the services they receive will be 'in-network'
and covered by their insurance. But often a doctor not in their insurance network is under contract with the hospital and
actually provides the care. When this happens, patients are stuck with unexpected and sometimes unreasonably high medical bills charged
by these 'out-of-network' doctors. This typically occurs when the hospital has outsourced the ER or other specialized services to
a professional staffing firm or a specialty doctors' practice. This problem has exploded in recent years because hospitals are increasingly
outsourcing these services to cut costs.
And more and more patients are faced with surprise medical bills -- adding substantially
to the already impossible medical debt that working people face. Hospital outsourcing of emergency, radiology, anesthesiology, and
other departments has provided an opening for physician practices to operate these services as independent organizations. Initially,
hospitals outsourced these services to small, local doctors' groups
But over the past decade, private equity firms have become major players -- buying out doctors' practices and rolling them up
into large corporate physician staffing firms that provide services to outsourced emergency rooms, anesthesiology and radiology departments,
and other specialty units. By 2013, physician staffing firms owned by Blackstone Group and Kohlberg, Kravis Roberts & Co. (KKR)
– among the largest PE firms in the country – cornered 30 percent of this market. Since then, private equity ownership of these services
has continued to grow.
Private equity firms also own two of the three largest emergency ambulance and air transport services – another major source of
surprise medical billing. Private equity ownership matters because the business model of private equity firms is to use a lot of
debt in a leveraged buyout of companies they acquire and then extract as much cash as possible out of them in order to pay down the
debt and reward their investors with 'outsized returns' that exceed stock market gains. They can be thought of as for-profit corporations
on steroids. Buying up specialty practices is financially attractive because there is a large and growing demand for outsourced doctors,
and out-of-network doctors can command a substantial premium for their services.
Emergency rooms and certain medical services provided in hospitals are not really part of a competitive 'marketplace' because
patients in emergency medical situations rarely have a choice: they need immediate medical care and cannot 'shop around' for an in-network
trauma doctor or radiologist.
Thus, surprise bills are difficult to avoid if patients face a medical emergency and must go to the ER or if they are hospitalized
and require access to specialty medical services. How Widespread is Surprise Billing and Why Has It Grown?
Surprise medical billing is exacerbating the already serious problem of medical debt in this country, which is a leading cause
of bankruptcy for American families.
[i]
And surprise billing is growing rapidly. Forty percent of Americans surveyed by the Kaufman Family Foundation in April, 2019,
reported receiving an unexpected medical bill; and 20 percent of those surveyed said it was due to out-of-network charges – or surprise
billing.
[ii]
A study by health researchers at Stanford University, for example, examined fees charged to patients with private insurance who
were treated by the emergency department of a hospital. They reviewed 13.6 million trips to the ER that occurred over the period
2010 to 2016. About a third (32.3 percent) of these trips in 2010 resulted in a surprise medical bill. But by 2016, that figure had
increased to 42.8 percent. That is, more than 4 in 10 trips to the ER ended with patients getting a surprise medical bill.
[iii]
For in-patient stays, surprise billing rose from 26 percent to 42 percent, and the average costs per patient also jumped from
$804 to $2,040. At this rate of increase, the estimated percent of hospital visits resulting in a surprise bill would be 48 percent
in 2019 – or almost one half.
The study also found that in 2016, 86% of ER visits and nearly 82% of hospital admissions incurred surprise ambulance service
bills. Similarly, another 2019 study found that patients who are admitted to a hospital from the ER are much more likely to receive
an out-of-network charge -- as many as 26% of admissions from the emergency room were found to include a surprise bill. The study
also found that 38 percent of Americans are 'very worried' and another 29 percent are 'somewhat worried' about being able to afford
surprise medical bills.
People particularly vulnerable to these charges are those with coverage from large employers that are self-insured. And vulnerability
also varied by region, with Texas, New York, Florida, New Jersey, and Kansas having higher rates of surprise billing; and Minnesota,
South Dakota, Nebraska, Maine, and Mississippi having lower rates.
[iv]
While large surprise medical bills are typically associated with doctors in the ER or in specialties such as radiology, anesthesiology,
or critical care units such as neo-natal, burn, or trauma centers, other out-of-network physicians may also issue surprise bills.
For example, those who assist a patient's doctor in a procedure or hospitalists who check on patients during hospital stays can also
charge separately for their services.
The Stanford study found that the likelihood that a patient admitted to an in-network hospital would face a surprise medical
bill because at least one out-of-network doctor cared for them increased from 26.3 percent 2010 to 42.0 percent in 2016. A particularly
egregious instance occurred when an assistant surgeon sent a bill for $117,000 to a patient who had surgery for herniated discs in
his neck.
The patient's own in-network surgeon sent a bill for $133,000, but accepted a fee of $6,200 negotiated with the insurance company.
The out-of-network assistant surgeon is seeking full payment of his charges. This is a particularly egregious example, but surprise
bills for a few thousand dollars are not uncommon.
[v]
The problem of surprise billing has grown substantially in recent years because hospitals have been under financial pressure to
reduce overall costs and have turned to outsourcing expensive and critical services to third-party providers as a cost-reduction
strategy. Outsourcing is not new, as hospitals began outsourcing non-medical ancillary services such as facilities management and
food services in the 1980s, in response to a round of structural changes in government financing.
By the 1990s, hospitals were experimenting with the use of independent 'hospitalists' to care for patients between rounds by the
local admitting doctors who had a hospital affiliation. Hospitalists' numbers increased over the next two decades as hospital staffing
firms grew and provided a range of temporary or short-term professionals to fill shortages in nursing, technical, or clinical positions.
[vi]
Recent outsourcing, however, has expanded to critical care areas – emergency rooms, radiology, anesthesiology, surgical care,
and specialized units for burn, trauma, or neo-natal care. Now hospitals contract with specialty physician practices or professional
physician staffing firms to provide these services – even if the patient receives treatment at a hospital or at an outpatient center
that is in the patients' insurance network. According to one study, surprise billing is concentrated in those hospitals that have
outsourced their emergency rooms.
[vii]
A recent report found that almost 65 percent of U.S. hospitals now have emergency rooms that are staffed by outside companies.
[viii]
Hospitals and healthcare systems have accelerated their outsourcing of critical care areas since 2010 in part due to declines
in Medicaid and Medicare reimbursements and to incentives under the Affordable Care Act to reduce costs and improve care quality.
[ix]
At the same time, on the supply side, hospitalist companies were merging and buying up practices of specialists employed mainly
in hospitals. Hospitalist companies evolved into physician staffing firms and expanded to include staffing for emergency rooms (ERs),
anesthesiology and radiology departments, and burn and neonatal intensive care units in hospitals across the country. The business
case for hospitals to outsource was straightforward. Emergency rooms are a major point of entry for patients who are admitted to
hospitals, and thus, a major conduit for the in-patient hospital stays that are critical for hospital revenue generation. But they
are costly and difficult to manage as they must be adequately staffed on a 24/7 basis regardless of patient flow, which is unpredictable.
Outsourcing the management, staffing, and billing of ER services shifts these management problems and the risk of underpayment for
these services to the staffing firm or a specialty doctors' practice. Hospital emergency rooms cannot turn patients away if they
lack adequate insurance coverage or any insurance at all; they must treat all patients. Emergency departments make money on ER visits
of patients with commercial insurance, but lose money on those with Medicare or Medicaid, and see very high losses when patients
have no insurance.
[x]
Private Equity's Business Model: Its Role in Outsourcing and Consolidating Specialty Services Private equity firms have played
a critical role in consolidating physicians' practices into large national staffing firms with substantial bargaining power vis-à-vis
hospitals and insurance companies. They have also bought up other emergency providers, such as ambulance and medical transport services.
They grow by buying up many small specialty practices and 'rolling them up' into umbrella organizations that serve healthcare systems
across the United States. Mergers of large physician staffing firms to create national powerhouses have also occurred. As these companies
grow in scale and scope and become the major providers of outsourced services, they have gained greater market power in their negotiations
with both hospitals and insurance companies: hospitals with whom they contract to provide services and insurance companies who are
responsible for paying the doctors' bills. Hospitals have consolidated in order to gain market share and negotiate higher insurance
payments for procedures.
Healthcare costs have been driven up further by the dynamics associated with payments for out-of-network services. As physicians'
practices merge or are bought out and rolled up by private equity firms, their ability to raise prices that patients or their insurance
companies pay for these doctors' services increases. The larger the share of the market these physician staffing firms control, the
greater their ability to charge high out-of-network fees. The likelihood of surprise medical bills goes up, and this is especially
true when Insurance companies find few doctors with these specialties in a given region with whom they can negotiate reasonable charges
for their services. The design of the private equity business model is geared to driving up the costs of patient care. Private equity
funds rely on the classic leveraged buyout model (LBO) in which they use substantial debt to buyout companies (in this case specialty
physician practices as well as ambulance services) because debt multiplies returns if the investment is successful. They target companies
that have a steady and high cash flow so they can manage the cash in order to service the debt and make high enough returns to pay
their investors 'outsized returns' that exceed the stock market.
[xi]
Emergency medical practices are a perfect buyout target because demand is inelastic, that is, it does not decline when prices
go up. Moreover, demand for these services is large – almost 50 percent of medical care comes from emergency room visits, according
to a 2017 national study by the University of Maryland School of Medicine, and demand has steadily increased.
[xii]
PE firms believe they face little or no downside market risk in these buyouts. Private-equity owned companies differ from publicly
traded for-profit chains not only in their greater use of debt, but also because the private equity firm, via the general partner
of the investment fund it sponsors, makes all investment decisions on behalf of the investor shareholders. Investors commit capital
to a PE-sponsored fund, typically for 10 years, and have no say in investment decisions. Thus, the PE general partner's power is
concentrated and largely unaccountable, as investors cannot 'exit' or sell their shares if they are dissatisfied – unlike shareholders
in publicly traded corporations.
[xiii]
In addition, PE firms charge their portfolio companies additional 'advisory fees' and 'transactions fees' that can amount to millions
of dollars over time. And because PE owned companies are not publicly traded on the stock exchange, they are not required to file
a detailed report to the Securities and Exchange Commission (SEC) the way that publicly traded companies must do. Their activities
and their financial transactions are largely hidden from the public eye, despite the fact that they receive substantial taxpayer
funding from Medicare and Medicaid for their services, though not for surprise charges. Two private-equity owned physician-staffing
firms dominate the market for outsourced doctors' practices -- Envision Healthcare, owned by KKR with 69,300 employees, and TeamHealth
owned by Blackstone Group with 20,000 employees. KKR also is a major owner (along with other private equity firms) of AirMedicalGroup
Holdings -- one of the nation's three largest ambulance and air transport companies.
We also showcase private equity owned Air Methods medical transport company. These examples help illuminate how and why private
equity firms have become national powerhouses in the provision of professional healthcare services and why their activities and those
of other private equity firms in this sector are leading to higher healthcare costs for patients and the industry as a whole.
Envision Healthcare
Envision Healthcare today is the result of fifteen years of private equity transactions in buying up and consolidating emergency
ambulance and specialty physicians' practices. It was formed in 2005 when private equity firm Onex took over two companies -- American
Medical Response (AMR) and EmCare -- and merged them. In and out of private equity ownership since 2005, Envision most recently was
acquired by KKR in October, 2018 in a public to private leveraged buyout worth $9.9 billion. Its sprawling organization employs tens
of thousands of healthcare professionals; and it supplies doctors in 774 physician practices to hospitals and ambulatory surgical
centers throughout the United States. It provides ER doctors, anesthesiologists, radiologists, hospitalists, and other specialists
covering intensive care, medical, neo-natal, pediatrics, psychiatric, skilled nursing, rehabilitation, and other inpatient units.
Its outpatient ambulatory surgical arm (AMSURG) provides trauma and acute care general surgery in 260 facilities in 35 states.
[xiv]
Between 2005 and 2018, Envision provided two types of emergency medical services: an ambulance and medical transport business
through American Medical Response (AMR) and emergency physician staffing through EmCare Holdings.
Today, Envision focuses on physician staffing services as it sold the ambulance and transport business in a $2.4 billion leveraged
buyout in 2018 to another private equity consortium that still includes KKR (as we detail below). The prior ownership patterns of
AMR and EmCare were similar. American Medical Response was listed as a publicly traded company as of August 1992; and in February,
1997, it was acquired by ambulance company MedTrans, a subsidiary of Laidlaw International. At an undisclosed date between 1997 and
2005, PE firm Peak Capital invested an undisclosed amount in the company. Like AMR, EmCare Holdings was acquired by Laidlaw International
in the summer of 1997 and subsequently received an undisclosed amount of investment from PE firm Peak Capital.
Emergency physician practices figured prominently among EmCare's 10 acquisitions and 17 sister physician staffing and management
firms.
[xv]
In December 2005, just months after acquiring and merging AMR and EmCare, Onex brought Envision Healthcare to the public market
via an IPO in which it retained a majority of the shares. Subsequent sales of shares left Onex with 31 percent of the company's equity
at the time it was again taken private, this time by Clayton Dubilier & Rice with participation of PE firm Ardian through a $3.2
billion LBO in May 2011. An IPO in 2013 returned Envision Healthcare to the public market. The PE owners retained about two-thirds
of the shares of the now-publicly traded company. The PE companies subsequently sold some of the stock. And in September 2017, two
hedge funds – Starboard Value and Comex Management – took minority stakes in Envision Healthcare.
Between July 2006 and October 2018, Envision Healthcare acquired 39 companies.
[xvi]
Envision Healthcare bought out AMSURG in December 2016 after AMSURG failed in an attempt to acquire TeamHealth (described below).
The deal brought together two seemingly complementary healthcare companies to form a single organization with pro forma market capitalization
of $10 billion and an enterprise value including debt of approximately $15 billion. A little over $8 billion of this was new debt.
However, KKR contributed $5.57 billion to the deal, using $4.43 billion to retire Envision's prior liabilities and the remainder
mainly as equity in the LBO.
Adding AMSURG's large chain of ambulatory surgical centers was supposed to make Envision Healthcare a dominant player across the
outsourced medical services landscape – emergency room doctors, hospitalists, outpatient surgery, and ground and air ambulance. But
integrating the two health care companies – with a combined 69,300 employees as of December 2017 – proved difficult for publicly
traded Envision Healthcare.
[xvii]
Envision Healthcare appears to be extremely profitable, but its financials are murky, with no publicly available accounting of
its transactions with each round of private equity buyouts. And under private equity ownership, when companies are taken private
or pass from one private equity fund to another, there is no transparency.
Each private equity buyout, however, is typically accompanied by levering substantial debt on the target company, which must be
serviced by managing for cash. Emergency medical services are attractive to private equity firms and are very lucrative because they
throw off a lot of cash, and as noted earlier, demand is inelastic and the fees are not subject to competitive market pricing. The
contracts negotiated between these physician staffing companies and hospitals also are not publicly available. Depending on how they
are crafted, they may provide incentives to outsource even more ER departments, and in turn increase out-of-network billing. One
Wall Street investor analysis, for example, highlights Envision's 'joint venture' model that raises serious questions.
A 2013 analysis by Deutsche Bank Securities described a 2012 joint venture between EmCare and the HCA Healthcare chain – with
a history of private equity ownership between 2006 and 2011 and substantial PE ownership of shares following its 2011 IPO. HCA apparently
agreed to give up directly charging for physicians' services and outsourced these services to EmCare in exchange for a 50-50 profit
split once EmCare achieved a 13% margin threshold, according to the Deutsche Bank calculation. This allowed EmCare to " penetrate
HCA's 160+ hospital portfolio more deeply with its physician offerings." As of 2014, EmCare valued its HCA joint venture at a net
revenue of $124 million, with assets of $155 million and liabilities of $31 million, according to the company's SEC filing. The filing
identified similar joint ventures with hospitals involving Evolution Health (also owned by Envision).
[xviii]
Commenting on EmCare's relations with hospitals, Benedic Ippolito, a research fellow in public finance and health economics
at the American Enterprise Institute, noted, "Right now, EmCare surprise bills patients and hospitals effectively turn a blind eye."
[xix]
Envision has come under heavy scrutiny for the huge out-of-network surprise medical bills it sends to ER patients.
A team of Yale University health economists examined the billing practices of EmCare, Envision's physician staffing arm.
[xx]
They found that when EmCare took over the management of emergency departments, it nearly doubled its charges for caring for patients
compared to the charges billed by previous physician groups. These egregious practices have resulted in a Congressional investigation
headed by Missouri Senator Claire McCaskill, lawsuits from shareholders, and court actions involving Envision and UnitedHealth Group,
the largest U.S. insurer.
[xxi]
TeamHealth
TeamHealth has also grown into a powerful national healthcare professional staffing company with 20,000 employees. It contracts
with hospitals to provide doctors and other healthcare professionals as ER staff, anesthesiologists, hospitalists, and hospital specialists
(OB/GYN, orthopedics, general surgery, pediatric services); and in post-acute care, ambulatory care, and behavioral health.
[xxii]
The company experienced successive rounds of private equity leveraged buyouts punctuated by IPOs that returned it to the public
markets – only to be taken private again through another LBO. In 1999, private equity firms Cornerstone Equity Investors and Madison
Dearborn Partners, with minority participation of Becken Petry O'Keefe and Company, acquired TeamHealth as a platform for a physician
staffing company. According to PitchBook (an industry research and data firm), TeamHealth acquired an anesthesiology practice, a
hospitalist company, and a health management business in its first two years. It made no further acquisitions until after it was
acquired by the Blackstone Group in 2005 in a leveraged secondary buyout (in which one PE fund sells a company to another PE fund).
TeamHealth made two more acquisitions between 2005 and 2009 – an emergency physician's group and a hospitalist company.
In 2009, Blackstone Group returned TeamHealth to the public market via an IPO, but retained possession of a majority of shares
in the newly public company. Passage of the Affordable Care Act in 2010, with its promise of cost containment via capitated and bundled
payments, spurred TeamHealth to go on a buying spree. Between 2010 and 2016, TeamHealth acquired 51 companies, mainly practices of
emergency doctors and anesthesiologists and a few hospital management companies. One very large exception to this pattern was TeamHealth's
2015 acquisition of IPC Healthcare.
[xxiii]
IPC Healthcare was a major hospitalist company. In its early years, it attracted four rounds of venture capital investments between
1998, when it was launched as IPC The Health Company, and 2002. In June 2002, IPC had an IPO and began its life as a publicly traded
company. Between 2002 and 2009, IPC acquired 20 physician practices. Between 2010 and 2015, following passage of the ACA, it acquired
78 more. The companies acquired by IPC were overwhelmingly hospitalist companies with a smattering of doctor's practices in specialties
such as geriatrics.
[xxiv]
TeamHealth's acquisition of IPC in 2015 raised questions. There was no evident fit between TeamHealth's specialty physician practices
and IPC's hospitalist companies. IPC was also in trouble with the Department of Justice, which in June 2014, had filed a civil lawsuit
against the company for "knowingly engaging in systematic overbilling" for services billed to Medicare and Medicaid and other government
health programs. Ultimately, TeamHealth paid $60 million plus interest to resolve these allegations.
[xxv]
This fueled speculation that TeamHealth, which had rebuffed AMSURG's attempt to acquire it, wanted this very large acquisition
in order to protect itself from being taken over. TeamHealth's explanation was that it wanted IPC's expertise in participating in
Medicare and Medicaid bundled payments programs.
[xxvi]
In February 2017, Blackstone Group once again took TeamHealth private in a $6.1 billion leveraged buyout. Similar to Envision
Healthcare, the financials of TeamHealth are murky. After many LBOs, its revenues, debt load, and financial stability remain unknown,
as do the contracts it negotiates with the phyisician groups it has acquired and the hospitals it contracts with for services.
And like Envision, its billing practices are being scrutinized. The Yale researchers who investigated EmCare and found excessive
use of surprise medical billing also examined TeamHealth's billing practices. They found that Blackstone owned TeamHealth has taken
a somewhat different tack. It uses the threat of sending high out-of-network surprise bills for ER doctors' services to an insurance
company's covered patients to gain high fees from the company as in-network doctors. In most cases, the researchers noted, TeamHealth
emergency physicians would go out-of-network for a few months, then rejoin the network after bargaining for in-network payment rates
that were 68 percent higher than in-network rates received by the previous ER doctors.
[xxvii]
While this avoids the situation of a patient getting a large, surprise medical bill for the services of ER doctors, it raises
healthcare costs and premiums for everyone.
Emergency Ambulance and Air Transport Services
Emergency ambulance and air transport is also a lucrative target for private equity investment, which has fueled consolidation
in this industry segment. Demand is inelastic – there is no competitive market pricing. And demand for air transport has grown considerably
because many rural hospitals have closed or consolidated, leading to far longer distances for access to emergency care. Two of the
three air transport companies that together control two-thirds of this US market are private equity owned – AirMedicalGroup Holdings
and Air Methods. The third, PHI Air Medical, is privately owned.
[xxviii]
Returning to the Envision story, recall that American Medical Response (AMR) was the ambulance service division that Envision
spun off in 2018. Before the divestiture, however, AMR grew to a national powerhouse in the decade from 2007 to2017 through 12 acquisitions
of ambulance and medical transport businesses and one air ambulance company7. In addition to these acquisitions, AMR has seven sister
companies – mainly ambulance companies, including several air ambulance businesses. It was acquired in 2017 by air ambulance company,
AirMedicalGroup Holdings (AMGH) -- owned by PE firms Ardian, Koch Equity Development, and KKR -- in a $2.4 billion leveraged buyout.
With this acquisition, AirMedicalGroup now holds a leading position in emergency and medical transport across a range of transport
modalities.
[xxix] The acquisition merged the largest provider of ground ambulance services in the U.S. with a leading operator
of medical helicopters, with over 320 locations in 38 states.
[xxx]
The combined entity creates the opportunity for KKR to substitute its more expensive medical helicopters for short trips previously
done by AMR's ambulances.
[xxxi]
Air Methods became private equity owned in 2017, when it was acquired by American Securities and Alpinvest Partners through a
$2.5 billion public-to-private LBO. The company's air medical transport services operate out of over 300 bases in 48 states.
[xxxii]
The buyout came in response to pressure from activist hedge fund investor, J. Daniel Plants, founder of Voce Capital Management.
Concerned about the bad publicity surrounding predatory charges by air ambulance companies, Plants wanted Air Methods to agree to
be taken private by a PE firm in order to keep information about its billing practices out of public view. According to the hedge
fund, Air Methods big price hikes created economic and political risks for the company. Going private would shield its financial
documents from patients and insurers. The hedge fund was right to be concerned about Air Methods predatory billing practices. The
average bill for being transported in one of its medical helicopters was $17,262 in 2009 and had risen to $40,766 in 2014. Air Methods
calculates that it accounts for nearly 30 percent of total air ambulance revenue in the U.S. Its profit increased sevenfold from
2004 to 2014.
[xxxiii]
In general, charges for out-of-network ambulance services are likely to be high. In the case of air ambulances, they are exceedingly
high – not only due to the high costs of air travel, but especially because an estimated 69 percent of charges are out-of-network
-- according to a 2017 US General Accountability Office (GAO) study of private insurance records for 2012-2017. That is, insured
patients in these cases ended up being billed for most of the charge. The GAO study also found that the median price for helicopter
service doubled between 2010 and 2014 – from roughly $15,000 to $30,000 per tri;p it also found that the average cost of an air ambulance
trip is over $36,000. .
[xxxiv]
Another study by researchers at Johns Hopkins University found charges were likely to be – as they put it – sky high. The study
found that air ambulance charges had risen substantially from 2012 to 2016, and in 2016 these charges ranged from 4 to 9 times higher
than what Medicare paid for this service. Some of the largest providers had among the highest charges. Between 2012 and 2016, the
median charge ratios (the charge divided by the Medicare rate) for the services increased by 46-61 percent.
[xxxv]
Legislative Solutions
Some hospitals have attempted to solve the problem of surprise billing on their own by simply requiring all attending physicians
in their hospitals to remain in-network – receiving payment from the insurance companies with whom the hospital has contracted. This
has been the traditional approach used by hospitals in managed care networks. According to John Cascell, Senior Vice President of
Managed Care at MemorialCare Health System in Fountain Valley, California, "Such stipulations were commonplace decades ago, but some
experts say the practice slipped out of favor around 2000 as major physician staffing companies -- which tend to make more money
when they're out of network -- gained market power."
[xxxvi]
MemorialCare, however, has retained this long-standing policy, which Cascell supports. The downside of this approach, however,
is that it may shift bargaining power to insurance companies who will seek to set lower in-network payments for specialty services.
In these cases, according to Cascell, MemorialCare takes a strong role in negotiating with insurance companies to maintain reasonable
payments.
[xxxvii]
More generally, the public, healthcare providers, insurers, and state and federal legislators recognize that individual solutions
are only stop-gap measures and that no individual hospital can solve the pervasive problem of surprise medical billing on its own.
Twenty-five states have passed legislation that aims to protect patients from surprise billing, but these laws do not fully cover
all types of situations. Over seventy-five percent of Americans believe that the federal government should step in and protect
them from surprise bills, according to a Kaufman Family Foundation April, 2019 national survey. The same survey found that 90 percent
of Democrats, three-quarters of Independents, and 60 percent of Republicans favored federal legislation to protect patients.
[xxxviii]
Americans differ, however, in who they think should bear the costs of care. According to the Kaufman survey, about half say insurance
companies alone should cover the costs of care (43 percent) while about half favor joint responsibility between providers and insurance
companies (47 percent).
[xxxix]
Two approaches to 'fixing' surprise medical bills have been put forward. One would benchmark the fees paid to out-of-network doctors
to the negotiated fees received by in-network doctors in that region for the procedure performed or the service provided. This would
have the effect of holding down health care costs by setting limits to what out-of-network physicians can charge. In the second approach,
out-of-network doctors would immediately be paid a given amount by the patient's insurance company – possibly 125 percent of the
Medicare payment or, alternatively, the median payment for that procedure or service in the geographic region – and could then take
the insurance company to arbitration in an effort to collect the balance of the patient's bill.
The second approach has the potential to raise health care costs if arbitration panels award out-of-network doctors all or a major
part of the fees they charge. This approach, which is favored by investor-owned physician staffing firms and by large physician practice
groups, would further raise health care costs for consumers. Even if many of these physician practices became in-network doctors,
as Envision now claims to be doing
[xl]
, the threat of going out-of-network remains. As the TeamHealth example illustrates, this allows physician staffing firms to
negotiate high in-network rates that drive up premium costs for consumers.
In sum, there is growing concern over the pricing practices of companies like Envision, TeamHealth, AirMedicalGroup, and Air Methods
-- leading emergency healthcare companies owned and operated by private equity firms. There is little oversight of the prices they
charge, and evidence suggests that these companies are among those responsible for driving up health costs by taking advantage of
the possibilities for surprise medical billing. But they are not alone, as private equity firms buy out medical services in specialties
other than trauma and radiology and as large physician practices take a page from the PE playbook when setting fees. Reining in these
charges is critical to efforts to slow the growth or even reduce health care costs.
[ii]
Ashley Kirzinger, Bryan Wu, and Mollyann Brodie. 2019. "KFF Health Tracking Poll – April 2019: Surprise Medical Bills and Public's
View of the Supreme Court and Continuing Protections for People with Pre-Existing Conditions." Figure 13. Kaufman Family Foundation.
April 24. https://www.kff.org/health-costs/poll-finding/kff-health-tracking-poll-april-2019/
(last accessed August 20, 2019)
[x]
Zack Cooper, Fiona Scott Morton and Nathan Shekita. 2018.
[xi]
For a detailed explanation of the PE business model, see Chapter 2, Eileen Appelbaum and Rosemary Batt. 2014. Private Equity
at Work: When Wall Street Manages Main Street , NY: Russell Sage Foundation Press.
[xii]
Jeff Lagasse. 2017. "Nearly Half of Medical Care Comes from Emergency Rooms, Study Shows."
[xiii]
Rosemary Batt and Eileen Appelbaum. 2019. "The Agency Costs of Private Equity: Why do Limited Partners Funds Still Invest?"
Academy of Management Perspectives. Forthcoming.
[xxvii]
Zack Cooper, Fiona Scott Morton, and Nathan Shekita. 2018.
[xxviii]
United States Government Accountability Office. 2019. "Air Ambulance: Available Data Show Privately-Insured Patients Are at Financial
Risk," GAO, March. https://www.gao.gov/assets/700 (last accessed
August 25, 2019)
[xxix]
PitchBook. 2019. American_Medical_Response_2019_8_10_13_21_18, American Medical Response Company Profile dated July 27, 2019.
[xxxiv]
United States Government Accountability Office. 2019.
[xxxv]
Ga Bai, Arjun Chanmugam, Valerie Y. Suslow, and Gerard F. Anderson. 2019. "Air Ambulances with Sky-High Charges," Health Affairs
, July: 38(7):1195-1200. https://www.ncbi.nlm.nih.gov/pubmed/31260345
(last accessed August 19, 2019)
[xl]
Envision's website states that it is committed to negotiating contracts for 'in-network status whenever possible.'
https://www.evhc.net/endsurprisecoverage (last accessed August
20, 2019)
"... our intelligent algorithm using state of the art innovative techniques of automation innovation disruption innovation disruption automatically sends orders to police and judges to prepare and serve pay or stay warrants, making sure your debtor goes to jail for their crime! ..."
"All 51 startups that debuted at Y Combinator W17 Demo Day 2" [
TechCrunch
]
(
day
one
). This is a good one:
Collectly helps doctors collect 2x's more debt than they have before. It's a business with
$280 billion sent to debt but the debt collectors only collect on average up to 20%. The founder
is a former CEO of a debt collection agency and collected over $100 million before
The acerbic Pinboard comments:
D Pinboard * Follow
@Pinboard
YC so far: surreptitious recording of phone calls, bus tickets for
the starving, debt collection, go live in a box, cow collars,
chatbots
Collectly
is some really depressing stuff. Wow. More from their website.
3. Transparent collection
Our intelligent software automatically reaches out to customers that didn't pay in
time, so you will never need to manually chase them again. And you can see every
action on every case.
Totaly fair.
Totaly fair? I had to read it twice. Is that a typo? Or does it mean something?
Next up:
our intelligent algorithm using state of the art innovative
techniques of automation innovation disruption innovation disruption automatically
sends orders to police and judges to prepare and serve pay or stay warrants, making
sure your debtor goes to jail for their crime!
Edit: Weird, this went in the wrong place. Oh well.
"... Record the names and phone numbers of the people you are dealing with. ..."
"... Document the date, time, and results of your phone calls. ..."
"... Pay something - even a small amount - on each bill each month as a gesture of good faith. ..."
"... Be aware, though, that some services charge high fees and do nothing to really help reduce your debt. ..."
"... Don't ignore bills. Though tempting, this is not a good strategy. Hospitals and providers are more likely to negotiate with you if you contact them immediately. ..."
"... Don't transfer debt to a credit card. Most experts warn that this is a poor choice for paying off medical debt ..."
Unless you have successfully challenged your bill, you are responsible for paying all of your medical
bills. If you cannot pay, here are some things to consider.
Try to negotiate a payment plan. Your hospital or provider may be willing to accept smaller
monthly payments. Keep in mind that your payments generally need to be reasonable and you must
keep up with your payments. In its
advice to parents of chronically ill children (link is external) , the American Academy of
Family Physicians recommends the following:
Notify the appropriate offices quickly.
Keep in touch with your creditors.
Record the names and phone numbers of the people you are dealing with.
Document the date, time, and results of your phone calls.
Pay something - even a small amount - on each bill each month as a gesture of good faith.
Apply for Wisconsin
Medicaid or
BadgerCare Plus
. If you are eligible, Medicaid may pay for some of your existing medical bills. Wisconsin
Medicaid coverage can begin as early as the first day of the month, three months before the month
you apply, if you would have been eligible in those months, so apply as soon as possible.
Go for credit counseling. Be aware, though, that some services charge high fees and do
nothing to really help reduce your debt. Make sure you are working with a credit counseling
service (also known as an adjustment service agency) that is licensed by the Wisconsin Department
of Financial Institutions.
A
list of licensed credit counselors (link is external) can be found at the Department of
Financial Institution's website. If you have questions or complaints about a particular agency,
call their Licensed Financial Services Section at (608)-261-7578.
Be creative about finding help from outside sources. Charitable foundations, civic organizations
and churches and community groups might be able to help. The
Patient Pal
(link is external) (PDF, 197 KB) from the
Patient Advocate Foundation (link is
external) includes some fundraising ideas for those with high medical bills.
Don't ignore bills. Though tempting, this is not a good strategy. Hospitals and providers
are more likely to negotiate with you if you contact them immediately.
Don't transfer debt to a credit card. Most experts warn that this is a poor choice for paying
off medical debt for two reasons:
The interest rates on your credit card will add significantly to your total payment.
Transferring medical debt to a credit card may affect your eligibility for Medicaid. Some
medical costs can be deducted from gross income to determine your Medicaid eligibility. Medical
debt on a credit card may no longer qualify as medical debt.
Dealing with collection agencies
If your hospital or other health care provider has turned your bill over to a collection agency,
you are protected against harassment by the Fair Debt Collection Practices Act (FDCPA).
Disputing a Debt (link is external) , from the Wisconsin Department of Financial Institutions,
provides information on how to deal with collection agencies.
If you have questions about your rights or the conduct of a collection agency, contact the Department
of Financial Institutions at (608) 264-7969, or 1-800-452-3328 (in Wisconsin only).
Medical debt collectors must abide by specific regulations, as set forth by the
Fair Debt Collection Practices Act . Collectors cannot harass or lie to debtors, or perform any
other practices deemed unfair.
You can get a free Kindle version of "Debt Collection Answers" ebook on Amazon
here .
Notable quotes:
"... We have heard from consumers who first hear about a medical bill from a collection agency. There is no federal law that protects you from this type of situation. ..."
Having even a small medical debt reported as past due or in collections can seriously damage your
credit history, you may be tempted to pay just to protect your credit.
Some medical providers may even try to pressure you into paying your debt owe by refusing to provide
you (or one of your family members) with additional medical care until you do. Some of them may even
refuse you future care while you are paying off your debt through an installment plan! Others may
have a policy that as long as you owe them money, you must pay up-front for all future medical services
they provide to you.
Warning: Aggressive medical providers can be a special problem for seniors living on fixed
incomes when their spouses have been hospitalized or have accumulated a large outstanding bill with
one or more of their doctors.
When Can I Be Sent to Collections On a Medical Bill?
If at all possible, you want to keep a medical bill out of collections. Once it is turned over
to a collection agency, it will likely appear on your credit reports as a collection account and
damage your credit rating.
Your medical debt may be turned over to collections:
If you are making payments. Even if you are making payments, you may find your account
turned over to collections with no advance warning . In addition, if you are late with a payment
under a payment agreement - even by one day - you may find your account in collections. There
is no federal law that stops a medical provider from turning an unpaid account over to collections
just because you are making payments.
While you are disputing a bill. If you have not paid a bill because you are disputing it,
or if you are waiting for your insurance company to pay it, beware! Your bill may be turned over
to collections with no advance warning.
If a medical bill remains unpaid - even if you never received a billing statement! We
have heard from consumers who first hear about a medical bill from a collection agency. There
is no federal law that protects you from this type of situation.
How can you protect yourself from medical debt collection? Don't ignore medical bills. Talk to
the medical provider. Get everything in writing, or follow up in writing yourself
... ... ...
If You Have Insurance and Your Insurer Refuses to Pay All or a Portion of Your Medical Bills
It's not unusual for health insurers to deny coverage for medical care. If that happens to you
and you believe that the care should be covered, or if your insurer pays some but not all of your
medical bill and you believe it should cover the entire bill, here's what we recommend:
Review your health insurance policy for an explanation of why the insurance company made the
decision it did.
If you don't find a good explanation in your policy, call the company's customer service office.
If you are unhappy with its explanation, contact your insurance agent or your health plan administrator,
if you receive your health insurance through your employer.
If your agent or the plan administrator is unable to help you with your claim, appeal the
decision of your health insurance company. Your agent or plan administrator can tell you how to
do that. At the same time, you may want to file a complaint against your insurance company with
your state's insurance commission or department, which may have a complaint resolution process.
Sometimes, filing this kind of complaint will make an insurance company rethink its approach to
a claim in order to avoid a problem with the state commission or department that is regulating
it.
Contact a consumer law attorney with experience in medical debt collection issues for help
if none of the actions you've taken have gotten you the results you had hoped for. Simply receiving
a letter from an attorney may get your insurance company to reverse its decision. It's also possible
that you may have to file a lawsuit against the company in order to get action. However, an attorney
will not take your case unless he or she thinks that you have a strong basis for a lawsuit and
a good chance of winning. If the attorney does, he or she will probably take your case on a contingent
fee basis, which means that you won't have to pay the attorney an up-front fee but instead, the
attorney will be paid by taking a share of whatever money he may win for you.
"... The CFPB says debt collection is a multi-billion dollar industry affecting 70 million consumers. People are most often contacted about medical and credit card debt. And more consumers complain to the CFPB about debt collection than any other financial product or service. ..."
"... Debt collectors can contact you by phone, letter, email or text message, as long as they follow the rules and disclose that they are debt collectors. It's against the law for a debt collector to pretend to be someone else to harass, threaten or deceive you. ..."
"... Collectors cannot lie to collect a debt, by falsely representing themselves or the amount you owe. And other than trying to obtain information about you, such as a telephone number or whereabouts, a debt collector generally is not permitted to discuss your debt with anyone other than you, your spouse, or your attorney. ..."
"... Also when you pay them off keep the document marked paid in full or zero balance or whatever else the send you on file including your financial proof (canceled check, money order, credit card receipt) keep it until you die! ..."
"... Debt industry buys billions of dollars of dead debt. 90% does end up as default judgement because scared debtors do not have the money to hire a attorney or do not know what to do. The other 10% of debtors who hire attorneys are off the hook. ..."
"... Consumer debts are self inflicted foolishness, medical debts aren't, but just goes to show the Empire is ran by business interests who refuse to allow any type of universal medical and have installed a system that allows them profits for illness and death ..."
A new Consumer Financial Protection Bureau report found that more than one in four consumers felt
threatened when contacted by debt collectors. The first-ever national survey of consumer
experiences with debt collectors found consumers often faced calls that came too often, at odd
hours and contained warnings of jail time and other threats. Some were contacted for debts they
didn't owe. And many said when they asked the collector to stop contacting them, the request was
ignored.
CFPB Director Rich Cordray said the report casts a "troubling light" on the industry, and that
the bureau is working to stop abuses. But what are your rights when facing off with a debt
collector?
A few things to know:
YOU ARE NOT ALONE
The CFPB says debt collection is a multi-billion dollar industry affecting 70 million
consumers. People are most often contacted about medical and credit card debt. And more consumers
complain to the CFPB about debt collection than any other financial product or service.
The Federal Trade Commission, which enforces the Fair Debt Collection Practices Act, also said
debt collectors generate more complaints to its offices than any other industry. While many debt
collectors are careful to comply with consumer protection laws, some engage in illegal practices.
YOU ARE PROTECTED
The Fair Debt Collection Practices Act provides protection for those being pursued for personal
debts, such as money owed on a credit card account, an auto loan or a mortgage. It doesn't cover
debts incurred to run a business.
YOU HAVE RIGHTS
Debt collectors can contact you by phone, letter, email or text message, as long as they
follow the rules and disclose that they are debt collectors. It's against the law for a debt
collector to pretend to be someone else to harass, threaten or deceive you.
They may not contact you at inconvenient times or places, such as early in the morning or late at
night. And they may not contact you at work if they're told not to.
Debt collectors may not harass, oppress, or abuse you, according to the FTC. That includes
threats of violence or using obscene language. Federal law also limits the number of calls a debt
collector can place.
Collectors cannot lie to collect a debt, by falsely representing themselves or the amount you
owe. And other than trying to obtain information about you, such as a telephone number or
whereabouts, a debt collector generally is not permitted to discuss your debt with anyone other
than you, your spouse, or your attorney.
YOU CAN TAKE ACTION
Report any problems you have with a debt collector to your state Attorney General's office, the
Federal Trade Commission and the Consumer Financial Protection Bureau. Many states have their own
debt collection laws that vary from federal law, so contact your attorney general's office for
help.
Gary G
They are debt collectors the lowest form of bottom feeding #$%$ on the planet.step one,
NEVER tell them any personal information whatsoever.step two, get a phone number and case
number so you can call them back.step three call them from a phone that can record the
conversation (theres an app for that)step three, call them when you are really ready to talk
to them Inform them the call is being recorded. let them know clearly what forms of contact
are and are not acceptable.step four, get the pertinent information about the debt including
the debtor any account numbers and any settlement offers they have. Still NEVER give away any
personal information. once you have all the information you need end the call, if at any time
during the call you feel you are being harassed or intimidated inform them it is not
acceptable (remember you are recording the conversation) and terminate the call. call back
later.Now you are in control and can make informed decisions.If at some point you want/need to
work out a settlement NEVER finalize anything on the phone, GET IT IN WRITING. NEVER, agree to
give them your credit card or banking information under any circumstances!!!once you make an
arrangement keep the printed document with the arrangement on file for the rest of your life.
Also when you pay them off keep the document marked paid in full or zero balance
or whatever else the send you on file including your financial proof (canceled check, money
order, credit card receipt) keep it until you die!
steven
Based on personal experience, the worst debt collectors are of the medical variety. Two
years of a fatal ovarian cancer case overwhelmed not only my finances, but jeopardized my
mental health as well. The only thing that kept me going was the necessity of showing up for
work, and the support of coworkers and (may I say this?) my managers as well.
Mark
Consumer Financial Protection Bureau will be gutted under the GOP agenda. So the next time
some cable company, Wall Street bank, or some other huge corporation screws you over, you'll
have no recourse and you'll be on your own.
pfk
I find tgheses stories and the ads on TV (If you owe $1000 to IRS..., If you have more than
$5,00 credit card debt, Reduce $50,00 debt to $5000..., etc) to e morally contemptible. If you
cannot afford something do not buy it; if you have a job, pay your IRS taxes, etc. I'm tired
paying extra for everything I buy or do for these people who spend and expect someone else
(me) to pay.
a
hogwash! To scare off a junk debt buyer attorney all you need to do is make one call to
your attorney. Many of you collectors "start fake lawsuits" to coerce debtors to pay. With no
filing numbers, court stamps, etc... Once the debtor's attorney files a 'notice of appearance'
and asks for a real lawsuit/trial, what happens? The creditor never files the lawsuit. Why?
Because the junk debt buyer has to PROVE IT. The JDB creditor has no original contract signed
to prove the debt exists, no chain of assignment/invoice to show they have standing to sue
(own the debt) nor the account statements to verify what is owed. They are hoping at best for
default judgements.
Debt industry buys billions of dollars of dead debt. 90% does end up as default judgement
because scared debtors do not have the money to hire a attorney or do not know what to do. The
other 10% of debtors who hire attorneys are off the hook.
You see Junk Debt Buyers buy
debt with no contract signed by debtors, have no invoice they even own this particular debt in
detail and no account statements to verify correct amount owed.
So debtors, beware, pay the few hundred dollars to your attorney to ask for a lawsuit and
notice of appearance and see how fast that debt collector disappears. 99% of junk debt
buyers/creditors buy unwarranted debt and CAN NOT PROVE IT IN COURT. There is a disclaimer on
the debt stating there is no contract, invoice that it is sold nor account statements offered.
Just sue these junk debt buyers and they go away. If they sell the debt to another JDB again
sue again and they drop the debt again. Resold debt has even less chance of winning in court
because even less proof is available every time it is sold.
But DO NOT AVOID the fake lawsuit. If you do the creditor gets the default judgement and will
garnish wages, lien your house, and will win. Now if the original creditor files the lawsuit
you will most likely lose and owe (they have all the proof in their records). So in this case
make a settlement offer of lump sum repay or payments you can afford.
Call me scum or whatever but I have used this strategy and it works. After a few decades of
paying usurious interest rates I have some cash finally coming back; and no need to file
bankruptcy. After 7 years it drops off your credit report and credit score goes way up. Make
it anywhere to 4-7 years (depending on your state law timeframe) and the statute of
limitations kicks in and money not legally owed any longer. Just do not make any payments on
it to renew statute of limitations. No problems! Hell I gambled the money away anyway, how was
I suppose to get it back -Ha, Ha. Joke was on the JDB in my case!
Gregory
Very poor article. Take it from some one who was being threatened for some one else's debt.
A certified letter to the debt collector explaining you do not owe the debt means that once
they receive the letter they can no longer contact you.
Violation of that law carries a 10,000 dollar fine. If the amount is in dispute the same
tactic works, except they can contact you with the proof of what you owe. A lot times this
involves too much work and they do not pursue it. So if they do not pursue it once the Statute
of Limitations is over the debt can no longer be collected.
The limit varies by State Law and amount. Finally be aware that uncollected debts are often
sold and the new "owner" of the debt may try to collect on it. Again a certified letter stops
them as you have proof of notification that the debt is not owed. I hope this helps the
victims out there.
Chub
Buying debt has become a large industry that attracts a lot of crooks. Companies buy debt
for as little as a dime on the dollar! The original lender benefits because they are getting a
little something out of a debt that they have no hope of collecting. The buyer of the debt
benefits because the potential profit is very
Many of the people buying debt aren't your traditional debt collection agency. They are many
times just an individual with a cell phone who could bend the rules because they can change
their name and location as easy as you can report their activity. Many times you are just
dealing with thugs with cellphones. If you owe them, don't be afraid to offer a lesser amount
because they had bought the debt so cheap that they may still make a pretty good profit.
Chief_blamestormer
Realize that some debtors never borrowed a dime. It could be the result of a civil
judgement. If you think all civil judgements are fair, then have a look at the cases in your
local courthouse, or serve a couple rounds of jury duty.
W,
19 hours ago
Industry? There's nothing industrious about. Bill collectors are mostly thugs who can't get
real jobs so they have to leverage their values off other people's misery.
Consumer debts
are self inflicted foolishness, medical debts aren't, but just goes to show the Empire is ran
by business interests who refuse to allow any type of universal medical and have installed a
system that allows them profits for illness and death
, which is similar to a developing
country, not a developed superpower.
"... Balance billing is on the rise nationally. In 2011, around 8 percent of privately insured individuals used out-of-network care, 40 percent of which resulted in unanticipated medical costs due to balance billing, reports Health Services Research . ..."
"... Balance billing complaints are up 1,000 percent in Texas . ..."
"... The rise in balance billing is partially attributable to a lack of network transparency with patients. ..."
"... The New York Times ..."
"... Kaiser Health News ..."
"... In 2014 Aetna sued a physician at Monmouth Medical Center in Long Branch, N.J., a hospital within Aetna's network, who did not notify a patient he would not accept Aetna's discounted reimbursement rate, according to the lawsuit. The physician charged Aetna $31,939 to treat abdominal pain in the patient. After Aetna paid the amount it deemed reasonable - $2,811, based on Medicare rates - the physician balance billed the patient for an additional $10,635. ..."
Patients, caught in the financial crosshairs, often feel powerless to negotiate costs. Consumer
advocacy groups and federal and state legislators are turning their attention to balance billing
practices this year with renewed vigor, forcing payers and providers to find other ways to settle
financial disagreements.
Here are 20 things to know about balance billing.
1. Balance billing is on the rise nationally. In 2011, around 8 percent of privately insured individuals
used out-of-network care, 40 percent of which resulted in unanticipated medical costs due to balance
billing, reports
Health
Services Research . In 2015, a nationwide study from
Consumers Union found nearly one third of privately insured Americans received an unanticipated
bill when their health plan paid less than expected for medical services within the past two years.
2. Balance billing complaints are up 1,000 percent in Texas . According to the
Texas Department of Insurance , balance billing complaints rose from 112 in 2012 to 1,334 in
2015, an increase of 1,000 percent.
3. Lack of provider, network transparency. The rise in balance billing is partially attributable
to a lack of network transparency with patients. In many cases patients are unaware they have received
out-of-network care until they receive a balance bill in the mail. Nearly 70 percent of individuals
with unaffordable out-of-network medical bills did not know the healthcare provider was not in their
plan's network at the time of care, according to a survey conducted by
Kaiser Family Foundation and The New York Times .
4. Emergency room services to blame, in part. A
Health Services Research survey found in 2011, 68 percent of inpatient involuntary contact with
out-of-network physicians was related to emergency care. These kinds of unanticipated medical bills
may arise when a hospital participates in an insurer's network but its employed emergency physicians
do not. For example, more than half of the hospitals in some Texas insurers' networks did not have
a single physician on staff covered by the insurer, according to a 2015 study from the Centers for
Public Policy Priorities in Austin.
5. Balance billing and contracted physicians. Many hospitals use physician outsourcing firms for
anesthesiologists, emergency physicians, pathologists and radiologists, or will bring in an outside
assistant surgeon to help with procedures. In many cases, these physicians do not participate in
the same network as the hospital, unbeknownst to the patient. When physician groups and insurers
are unable to resolve reimbursement disputes, patients can be served with much higher out-of-network
charges. In Texas, for example, the specialty services most likely to submit balance bills are anesthesiologists,
lab services, surgery and radiology, reports the
Texas Department of Insurance .
6. Payers will fight out-of-network physicians with lower reimbursement rates. Last year, health
insurance giant UnitedHealthcare said it would scale back how much it pays out-of-network physicians
who practice at in-network hospitals, accusing physicians of demanding excessively high reimbursement
levels, according to
Kaiser Health News . During a
billing dispute with out-of-network Bayonne (N.J.) Medical Center, the insurer accused the hospital
of charging out-of-network rates 10 to 12 times higher for a medical service than area hospitals
participating in United'snetwork. If a payer refuses to match physician reimbursement rates, the
financial burden is passed on to the patient. In the aforementioned dispute between Bayonne and UnitedHealthcare,
the patient was balance billed $1,170 for a total of five stitches.
7. Insurers are narrowing networks in an effort to reduce costs. As insurance companies have narrowed
provider networks to keep premiums down, the number of patients who inadvertently received
out-of-network care has jumped at hospitals, particularly with regard to contracted physicians.
8. Payers have sued providers for 'excessive' out-of-network fees. Aetna
has sued a half dozen out-of-network physicians in recent years, alleging gross over charging
for medical services. In 2014 Aetna sued a physician at Monmouth Medical Center in Long Branch, N.J.,
a hospital within Aetna's network, who did not notify a patient he would not accept Aetna's discounted
reimbursement rate, according to the lawsuit. The physician charged Aetna $31,939 to treat abdominal
pain in the patient. After Aetna paid the amount it deemed reasonable - $2,811, based on Medicare
rates - the physician balance billed the patient for an additional $10,635.
9. Balance billing can occur even when a payer adjusts out-of-network emergency bills to in-network
rates for patients. A patient recently accused Duke University Medical Center in Durham, N.C., of
balance billing his account for an out-of-network rate after the patient submitted in-network payment
rates to Blue Cross Blue Shield. Owing to the medical emergency of his situation,
Matthew
Aitken said he received an in-network rate from Blue Cross Blue Shield of North Carolina. However,
Mr. Aitken alleged Duke proceeded to charge him for the remainder of the bill at the higher out-of-network
rate, resulting in a bill nearly double that of Mr. Aitken's out-of-pocket limit.
10. Air ambulance billing disputes, complaints on the rise. In rural areas of the U.S. the high
price for life-saving
air ambulance flights has grabbed media attention as rural residents, faced with excessive balance
billing, have turned to state and federal auditors for intervention. Those in rural areas often must
rely on air ambulance flights in life-or-death situations in lieu of feasible ground transportation.
Reimbursement rate disputes between payers and medical air transport companies have strapped patients
with devastating medical bills. When Amy Thomson's newborn daughter was in heart failure, Ms. Thomson
had to use an air ambulance service in rural Montana for transport to a more capable facility. At
the time her insurance company, PacificSource, did not have an in-network air ambulance company near
her family, reports
Montana Public Radio . Ms. Thomson received a $43,000 balance bill from Airlift Northwest
after PacificSource contributed a policy cap of $13,000.
11. Provider-based billing practices. Consumers have been increasingly vocal about surprise medical
bills derived from
provider-based billing practices. Provider-based billing allows a healthcare organization to
bill patients for physician care in addition to a service charge for the patient's use of hospital
facilities and equipment. In some cases, a patient may be responsible for the service bill if their
insurance declines to pay or if the patient has a high deductible health plan. Large hospitals like
Cleveland Clinic have faced increased scrutiny for provider-based billing practices. After paying
a $30 copayment for in-network care with a Cleveland Clinic chiropractor,
Julie Beinhardt reported receiving a balance bill of $3,000 for provider-based service fees her
insurance plan refused to cover.
12. President Barack Obama signed legislation against provider-based billing. Last year, President
Obama signed
legislation outlawing provider-based billing at off-campus outpatient facilities. The legislation
does not apply to existing outpatient centers that already engage in the practice, however.
13. The president's 2017 budget proposal includes a provision to eliminate surprise medical bills.
Although details are minimal, the president's 2017 budget proposal includes a provision to eliminate
balance billing privately insured patients. The administration would address the issue by requiring
physicians who regularly provide services in hospitals to accept in-network rates for service reimbursement,
even if they aren't in the insurer's network.
14. About a quarter of U.S. states have laws that protect consumers from out-of-network medical
bills incurred by emergency care. According to a study from
Kaiser Family Foundation , 24 states have implemented laws that restrict providers from balance
billing in emergency care situations, including California, Delaware, New Jersey, New York and Pennsylvania,
among others.
15. More states are proposing independent dispute resolution between payers and providers in balance
billing cases. Independent dispute resolution establishes a legal space in which providers and health
insurers can settle disagreements regarding balance billing without involving the patient. The states
of
Illinois
and New Yorkhave arbitration methods in place, and
Florida ,
Washington and
Pennsylvania are currently considering a similar resolution methods.
16. New York has some of the strongest consumer protection laws. Under
New York law , consumers are generally protected from owing more than their in-network copayment,
coinsurance or deductible on bills they receive for out-of-network emergency services. Patients can
complete an assignment of benefits form that absolves them of financial responsibility and allows
the provider to pursue payment from the health plan in balance billing disputes.
17. Florida state legislature is currently embroiled in a fight to pass balance billing laws.
Legislation to outlaw balance billing in Florida has continued to creep through the state legislature
since last fall. Introduced in both the house and senate, the bills have sparked conflicting and
outspoken opinions from patients, payers, hospitals and physicians. Hospitals have largely denounced
the bill, blaming balance billing disputes on payers that demand allegedly unsustainable reimbursement
rates, reports
Sunshine State News .
18. The "End Surprise Billing Act". Federal lawmakers are making moves to outlaw balance billing
nationally. Co-sponsored by 25 lawmakers, the End Surprise Billing Act would protect patients from
balance billing who went to in-network facilities for emergency services, reports
Consumerist . In non-emergency cases, it would require providers to notify patients
within 24 hours if an out-of-network specialist will be involved in an episode of care.
19. Consumers don't know how to navigate the legal waters. According to a
Consumer Union report, 57 percent of patients who encountered balance billing from contracted
physicians within the last two years paid in full because they didn't know their rights to fight
the bills. An overwhelming majority (87 percent) did not know which agency or department in their
state government is tasked with handling complaints about health insurance. "So many times, people
just give up [in surprise billing disputes]," Elisabeth Benjamin, vice president of health initiatives
with Community Service Society of New York, told
NPR .
20. The New York Times dedicated a series to consumer encounters with surprise healthcare
bills. Elisabeth Rosenthal's series in The New York Times entitled
Paying Til it Hurts examined the personal and financial implications of excessive, unexpected
medical costs on Americans, their families and their healthcare consumption. Ms. Rosenthal's installments
often feature individuals with unaffordable balance bills like
Peter Drier , who was served a $117,000 balance bill for an out-of-network physician's assistant
he never knew was present during surgery.
The New Jersey Department of Banking and Insurance also prohibits physicians with a contractual relationship with a health
plan from balance billing HMO members and extends the ban on balance billing to out-of-network providers who treat HMO members
based on a referral from a participating provider or the HMO itself.13 After receiving a number of complaints concerning an
Aetna policy that purported that payments received by out-of-network providers be considered as payment in full, the Department
of Banking and Insurance ordered HMOs to "pay the non-participating provider a benefit large enough to insure that the non-participating
provider does not balance bill the member for the difference between his billed charges and the . . . payment, even if it means
that [the HMO] must pay the provider's billed charges less the member's network copayment, coinsurance or deductible."14 Here
too, HMO patients are completely insulated from financial responsibility, excepting any applicable copayments and deductibles.
Call TDI's Consumer Help Line at 1-800-252-3439 to discuss your options. There are two main ways TDI can help:
Mediation:
Texas law allows many consumers to seek mediation for bills that exceed $500. TDI has helped 94 percent of these consumers lower
their bills in the first stage of the process.
Complaints:
We helped recover $490,518 for Texas consumers who filed complaints about balance billing in 2015.
Complain to the right agency.
If you believe you've been treated unfairly, file a complaint with the agency that regulates your provider or health plan.
File complaints against doctors with the Texas Medical Board.
File complaints against hospitals, ambulatory surgical centers, or other facilities with the
How to File a Complaint - Health Facilities.
File complaints against licensed health maintenance organizations and health insurance companies with the Texas Department of
Insurance.
The Assembly Insurance and Financial Institutions Committee approved the bill by a 9-3 vote, although even supporters said they
had concerns about how the arbitration system would work.
"The arbitration is something we need to work out and resolve, but we are getting there and making great progress," Committee Vice-Chairwoman
Pamela Lampitt (D-Camden) said.
The bill (A1952) was praised by consumer advocates like Ray Castro of New Jersey Policy Perspective. An estimated 168,000 people
in the state receive an out-of-network bill they did not anticipate every year for an average $2,500.
... ... ...
"Surprise bills are driving up the cost of insurance and unfairly penalizing New Jerseyans who do all the right things -- buying
insurance and using in-network providers," said Maura Collinsgru, health policy advocate for N.J. Citizen Action, a consumer and
labor group.
The Assembly Financial Institutions and Insurance Committee approved the bill.
The bill would have little effect on self-funded, federally regulated insurance plans which are not bound by state law, representing
70 percent of New Jersey residents. Coughlin said self-insured companies may opt-in and will do so because they want to participate
in the arbitration process.
The committee also approved a companion bill, (A2866) that would create a healthcare price index containing billing claims data to
serve as a source for policy makers to monitor health care costs and efforts to contain them.
"Far too many New Jersey families -- even those with quality health benefits plans -- find themselves fighting over thousands of
dollars in out-of-network charges they never even had the opportunity to review, let alone agree to, prior to receiving medical attention,"
said Assemblyman Craig Coughlin (D-Middlesex), a sponsor of the bill and committee chairman.
I love how nobody ever mentions the fact that patients pay a premium to carry out of network benefits, yet the insurance companies
are paying less than Medicare rates to out of network providers! Where is the money going? It's the fact that the insurance company
chronically pays less on a given claim to the doctor forcing the doctor to charge more to the patient. This makes billed charges
overall (and therefore the cost to patients) go through the roof. The media (and insurance companies) want us to believe doctors
are greedy pigs for being out of network, but the in-network rates are so low it keeps doctors working non stop as they require
a larger volume of patients...therefore sacrificing a level of care to all those patients. The REAL VILLAINS are the insurance
carriers... so-called "non-profit" Blue Cross and the other money making machines (Aetna, United, Cigna.) Fair Health would be
FAIR to all if the insurance companies would agree to use it.
bigred, Jun 21, 2016
NJ has the highest health costs in the country so to say Doctors would leave the state is a joke. A federal study done on medicare
states that NJ has the highest bills; most people do not realize that Hackensack hospital has higher co pays than Columbia Presbyterian
in NY which is only ten blocks from the GW; I can attest due to personal experience and the care is better rated too.
The Thinker, Jun 21, 2016
It is indeed a sham that all hospital based physician employees do not accept the same healthcare plans as that of the
hospital. The unknown consequences however is that a plastic surgeon on staff but not working for the hospital might refuse
to come in if he cannot charge his fees. That is a big problem.
SleepingIn, Jun 21, 2016
@The Thinker Hmmm way to uphold the Hippocratic oath bub..I guess buying princess a new Mercedes is more important.
wondersunceasing, Jun 20, 2016
It is stupid that a doctor in a hospital does not accept all insurances that hospital accepts.....
Odds are good that balanced billing has adversely affected someone you know, even if the affected person hasn't realized it. It's
just so easy to pay a bill without first investigating it, especially if the overage being billed is small enough that we don't readily
notice. We should all check our bills with an eagle eye and compare what should be paid with what the provider is asking us to pay.
But if you live in a state like Arizona, you are going to need more than an eagle eye. You're going to need the power of the
vote. You are going to have to be proactive and vote for leaders who pay more attention to their constituents than they do to powerful
lobbies.
... ... ...
As a July, 2013
Becker's Hospital Review article shows, some hospitals make billions in profit. Yet they continue to charge huge fees for
even the smallest of goods and services. We've all heard the stories of that $1,000 toothbrush on the hospital's itemized list, and
sadly, it's not urban legend. It's real. And with medical costs spiraling out of control, patients are understandably leery, yet
left with nowhere to turn.
... ... ...
On the other hand, the issue is not cut and dried. Some hospitals barely break even or operate at a loss. And while hospitals
and doctors bill their patients at ever-rising rates, that practice may be done in part to offset the care they must provide to those
who can't pay at all. It's a vicious circle. But that viciousness should never be the problem of the insured patient. Insurance is
defined in its simplest terms as "protection". But when balanced billing is permitted, protection fails. Balanced billing will never
be the answer to the problem.
Balanced billing is an ugly parasitic beast of the insurance industry. And like most parasites, it can do great harm... unless
we choose to eradicate it.
Section 10101 of the Patient Protection and Affordable Care Act added numerous new patient protections to the Public Health Service
Act ("PHS Act"), including Section 2719A which, inter alia, requires group health plans that cover emergency services to provide
such coverage without the need for prior authorization, regardless of the participating status of the provider, and at the in-network
cost-sharing level.4
In order to implement Section 2719A of the PHS Act, the Secretaries of the Departments of Health and Human Services, Labor, and the
Treasury issued regulations that require the patient's group health plan to reimburse out-of-network emergency service by paying
"the greatest of three possible amounts - (1) the amount negotiated with in-network providers for the emergency service furnished;
(2) the amount for the emergency service calculated using the same method the plan generally uses to determine payments for out-of-network
services (such as the usual, customary, and reasonable charges); or (3) the amount that would be paid under Medicare for the emergency
service." While this addresses the payor's responsibility for emergency services in an emergency department of a hospital, the PHS
Act does not address all other out-of-network services or the balance billing of patients in excess of the health plan's responsibility.
Thus, "[o]ut of network providers may, however, also balance bill patients for the difference between the providers' charges and
amount collected from the plan . . ."5
Negotiating after-the-fact when you've gotten a legal balance bill is more difficult, but you still have options.
You can negotiate the balance-billed portion with your provider. Remember, your provider wants to get paid and would prefer to
get his or her money quickly and without having to pay a portion of it to a collection agency. This means a provider might agree
to decrease the total amount billed to the discount rate that she receives from the insurance companies she's in-network with, if
you agree to pay your share immediately. Or, your provider might accept a portion of the remaining balance as payment in full if
you agree to pay in cash immediately. Some will allow you to set up a payment plan.
You can negotiate with your insurer. If your insurer has already paid the out-of-network rate on the reasonable and customary
charge, you'll have difficulty filing a formal appeal since the insurer didn't actually deny your claim. It paid your claim,
but at the out-of-network rate. Instead, request a reconsideration. You want your insurance company to reconsider the decision
to cover this as out-of-network care, and instead cover it as in-network care. You'll have more luck with this approach if you
had a compelling medical or logistical reason for choosing an out-of-network provider.
If you feel like you've been treated unfairly by your insurance company, follow your health plan's internal complaint resolution
process. You can get information about your insurer's complaint resolution process in your benefits handbook or from your human
resources department. If this doesn't resolve the problem, you can complain to your state's Department of Insurance. Find
contact information for your Department of Insurance by clicking
your state on this map.
If your health plan is self-funded, meaning your employer is the entity actually paying the medical bills even though an insurance
company may administer the plan, then your health plan may not fall under the jurisdiction of your state's department of insurance.
Self-funded plans usually fall under the jurisdiction of the Department of Labor's Employee Benefit Services Administration. Get
more information from the EBSA's consumer assistance
web page or by calling an EBSA benefits advisor at 1-866-444-3272.
Perhaps the most monstrous thing about the American medical system - and the bar for that title is high indeed - is
predatory billing.
A great many medical providers adjust their prices based on how defenseless the patient is, and bleed the weakest ones for every
last red cent,
often with
preposterously inflated charges for things like aspirin and bandages. A 2015 study looked at the worst price gougers in the country
and found 50 hospitals that charged uninsured people roughly
10 times the actual cost of care.
Key to this practice is something called "balance billing," and it's why the American Medical Association is strongly supporting
Donald Trump's
pick of Rep. Tom Price (R-Ga.) to lead the Department of Health and Human Services, which oversees Medicare. Balance billing
is forbidden for Medicare enrollees, but Price wants to allow it - thus allowing doctors and hospitals to devour the nest eggs of
thousands of American seniors.
So what is balance billing? It's the practice of billing the patient for the difference between the sticker price and what insurance
will pay. So if a hospital visit costs $1,000, but your insurance will only cover $300, some providers will "balance bill" you for
$700.
For unscrupulous providers, the method of exploitation is obvious: When doing any sort of expensive procedure, take a rough estimate
of the absolute maximum the patient can pay, and jack up the price so the balance hits it. Or if you're short on time, just bill
them into the stratosphere, and you'll get whatever the patient has during the bankruptcy proceeding.
People being blindsided by immense out-of-network bills - going to an in-network hospital that employs an out-of-network surgeon
they conveniently failed to tell you about, for example - is an
increasingly common experience.
That is why ObamaCare failed to stop people
being bankrupted by medical debt (though it did slow medical bankruptcies substantially).
Permanently obliterating the financial security of helpless families with no or bad insurance as a loved one dies slowly and painfully
of a chronic illness is a nice little profit center for providers. But it pales in comparison to the gravy train they might get if
they can bring balance billing to Medicare. Seniors use far more care than the younger exchange population, and there are a lot more
of them - 55.5
million, versus
12.7 million people on the exchanges. Perhaps most importantly, they're quite a bit richer on average. Many seniors have been
scrimping their whole lives to save for retirement, in keeping with
decades of agitprop from
conservatives and Wall Street, and the more sociopathic among the health-care population are licking their chops at the prospect
of being able to devour those nest eggs.
That brings me back to Tom Price and the AMA. In 2011, Price (an orthopedic surgeon himself) introduced a Medicare "reform"
bill in Congress that, among other things, would have brought balance billing to the program. This would greatly increase
provider and physician revenues, and the
AMA eagerly lined up behind it.
Physician salaries are of course already none too shabby: An
average salary
for a primary care doctor in 2015 was $195,000; for specialists it was $284,000. Hey, a few thousand grandparents might lose their
retirement, but that fourth BMW isn't going to buy itself.
Now, balance billing on Medicare would not be quite so horrible as it is for uninsured people. Physicians would still have to
set up contracts beforehand setting an agreed price - they could not be simply be adjusted at will. But those contract prices are
guaranteed to be vastly higher than what Medicare pays now. It will be akin to seeing an out-of-network provider on private insurance
now, something that causes thousands of bankruptcies today.
Even in that attenuated form balance billing would also go no small distance toward abolishing Medicare as an actual program of
insurance. Medical debt-induced bankruptcies will become a routine occurrence for Medicare enrollees - how can you be said to be
insured if too much care might easily end up costing your entire net worth?
It's important to note that a great many doctors are
not on board with this plan. Most no doubt got into the business to help sick people, not loot the elderly at their weakest moment
in life. The AMA - which mobilized a
hysterical deluge of
red-baiting to kill President Truman's single-payer insurance plan in 1948 - is probably the most reactionary and selfish of
the doctor lobbying groups, but
even some of their membership
is rebelling at the idea of blowing a huge hole in Medicare. Other groups are dead against it.
But allowing balance billing in Medicare is a straight-up evil policy. Republicans will attempt to camouflage it as allowing
"free
contracts" between patients and doctors or similar nonsense. Don't believe a word of it, seniors. They want your retirement money.
Editor's note: A previous version of this article misdescribed balance billing's effect on Medicare. It has since been corrected.
We regret the error.
Balance billing is a controversial and often illegal practice in which your healthcare provider – usually a physician or hospital
– goes after you for money that you don't owe.
Balance billing may happen
when your health plan pays less than what your doctor or hospital charges and want to be paid. Your healthcare provider may demand
the balance of the bill from you. Unfortunately, some people do not know that this is inappropriate and, fearing a call from a debt
collector or a threat to their credit rating, pay what is being asked.
Balance billing usually happens when healthcare providers who participate in a
managed-care network or in Medicare believe
that the health plan is not paying enough for a medical service or is taking too long to pay. However valid the payment issue may
be, your doctor should only appeal to your health plan and not get you and other patients caught in the middle.
Is Balance Billing Always Illegal?
Balance billing is illegal for all approved Medicare services
provided by your doctor or hospital. Additionally, 47 states have laws that require doctors and other health providers who have a
contract with a health plan to seek payment only from that health plan and not from their patients.
These laws vary from state to state and may include only some types of health plans. Pennsylvania is a good example of a state
with a balance bill law that applies to most (if not all) healthcare providers – "it shall be unlawful for any health care practitioner,
or any primary health center, corporation, facility, institution or other entity that employs a health care practitioner, to balance-bill."
Balance billing does not include your doctor or other provider charging or collecting
out-of-pocket expenses such as deductibles,
copayments, or co-insurance that may be required by your health plan.
Your state's ban on balance billing usually does not apply if you have an elective procedure, such as cosmetic surgery, which
is not a covered benefit.
Additionally, you may be liable for the complete bill or a balance if you get an
out-of-network service that is not an emergency and
has not been approved by your health
plan.
Many states also protect members of health plans from balance billing in emergencies. If you have a medical emergency, you may
have no control over who treats you and where you are treated. For example, if you have a heart attack or are in a bad accident,
you may be taken to a hospital that is not in your health plan's network.
Do Health Plans Allow Doctors to Balance Bill?
If your doctor is part of a managed care network (and most physicians do belong to one or more networks) she has a contract with
your health plan that most likely prohibits her from sending you a bill in excess of your required
copayments. Typical contract language, for
example, often is worded as follows: "the provider agrees to accept the payer's network rate as payment in full for covered services
and shall not balance-bill the payer's subscribers."
If your in-network doctor bills you in violation of her contract, she could risk a financial penalty or cancellation of her contract
with the health plan. Even if your health plan does not prohibit balance billing, your doctor is still subject to any state laws
that ban balance billing.
How Can I Prevent Balance Billing?
The best way to prevent getting an inappropriate bill from a healthcare provider is to make sure that you fully understand your
health plan's rules and you know how to read and interpret the
explanation of benefits (EOB) sent by your
health plan or Medicare.
only using in-network doctors,
hospitals, and other providers (such as labs and x-ray facilities)
knowing what services are covered by your health plan
making sure to get prior authorization for a medical service, if required
When in doubt, call your health plan's customer service line for advice.
What Can I Do if I Receive a Balance Bill?
If you have any concerns that the bill you received is not appropriate, do not pay it. You have several options, including:
Call your health plan first and determine what your
payment responsibility
is. If you are in an HMO and received your service from a network doctor, your only responsibility should be your copayment. When
you call, have all the necessary paperwork, including your member number, the balance bill, and your EOB.
Call your doctor's office or hospital billing department and dispute the charges. When you call, make sure that you know what
your health plan's balance billing rules as well as laws in your state. Usually, you can find this information on the website
of your state's insurance department.
If you cannot resolve the issue with your health plan or doctor's office, file a complaint with your state's insurance department
or Attorney General. Your state may also have a consumer advocate office.
Also, you can consult a lawyer who specializes in medical billing disputes.
According to a study done in California in 2007 about 56% of people who received an inappropriate balance bill from an emergency
room paid it. The average bill was $300, meaning balance billing was a $528 million burden on patients with health insurance. This
is just for the state of California and only for emergency
room visits!
Although national figures are not available, some health economists and patient advocates estimate that consumers pay $1 billion
or more a year in balance billing for which they are not responsible.
Your doctor should be bickering with your health plan, not you! Do not pay a bill that you are not sure about until you
check with your health plan. And, if you owe the money, it is important that you pay your doctor – she has to pay office rent, the
cost of supplies, and staff salaries.
The Last but not LeastTechnology is dominated by
two types of people: those who understand what they do not manage and those who manage what they do not understand ~Archibald Putt.
Ph.D
FAIR USE NOTICEThis site contains
copyrighted material the use of which has not always been specifically
authorized by the copyright owner. We are making such material available
to advance understanding of computer science, IT technology, economic, scientific, and social
issues. We believe this constitutes a 'fair use' of any such
copyrighted material as provided by section 107 of the US Copyright Law according to which
such material can be distributed without profit exclusively for research and educational purposes.
This is a Spartan WHYFF (We Help You For Free)
site written by people for whom English is not a native language. Grammar and spelling errors should
be expected. The site contain some broken links as it develops like a living tree...
You can use PayPal to to buy a cup of coffee for authors
of this site
Disclaimer:
The statements, views and opinions presented on this web page are those of the author (or
referenced source) and are
not endorsed by, nor do they necessarily reflect, the opinions of the Softpanorama society.We do not warrant the correctness
of the information provided or its fitness for any purpose. The site uses AdSense so you need to be aware of Google privacy policy. You you do not want to be
tracked by Google please disable Javascript for this site. This site is perfectly usable without
Javascript.
ER doctors, anesthesiologists, radiologists and other specialists who typically charge out-of-network prices are among the highest-compensated practitioners. I have found this to be true during my hospital visits. If the insurance company can not convince them to take a lesser rate, you are stuck will the bill. I have been tempted to ask at the time of need whether they are all in network and employees of the facility I am visiting that day. Countering the argument by insurance, doctors, and hospitals complain healthcare insurance companies have the upper hand due to size and market control and can pay the increased costs of out-of-network pricing. As shown chart 1, their claims are not precisely true and the market for healthcare has become less competitive as hospitals and ACOs buy up the competition.
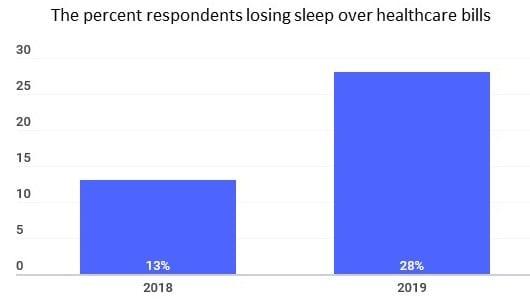
.